
Tag: sleeve gastrectomy
A patinet story: Lap Band complication and Wagovy
October 24, 2024 4:30 pm
Not too long ago, I saw an old patient who had seen me years ago after having had a lap band placed for weight loss. At the time, I recommended that the lap band be removed and that alternative plans be made. I suspected a slipped band. We discussed the reality that after the band removal, weight gain is to be expected. Several surgical options were discussed, and the patient dismissed them as “too radical.” The patient decided to “deal” with the ongoing nausea and vomiting since it was a small price to pay for the weight loss. I warned the patient that elective removal of the band is much safer than an emergency procedure in the middle of the night when it is least convenient. The patient did end up with an emergency lap band removal and was started on GLP-1 Agonists (Wagovy) because of the weight gain that followed the band removal. The side effects of the medication were debilitating, with nausea, dizziness, and fainting due to low blood sugar. The drug has all been stopped, and most, not all, of the side effects are resolved. The plan is to get this patient in a better shape and, reevaluate the esophagus and the stomach, and formulate a strategy based on the blood work, upper endoscopy, upper GI study findings and decide if the patient will be a good candidate for the Laparoscopic sleeve or the duodenal switch operation.
Here are my recommendations:
- Patients should avoid lap bands. Those with lap bands, regardless of how they feel and whether they are having issues with them, should have the lap band removed immediately before they end up in the emergency room or have irreversible changes to the cells or function of the stomach and esophagus.
- Patients who have the lap band removed will have less weight loss with the sleeve than those who have the sleeve as the primary procedure (the lesson here is that a less invasive, seemingly easy solution is much worse long term; more on this below). Lap Band patients should be revised to the duodenal switch, SPIS, SADI, or Gastric bypass if they have substantial weight to lose.
- GLP-1 agonist medication should be avoided. It is not a solution to the underlying problem but a band-aid covering the metabolic derangement.
- GLP-1 agonist medication needs to be taken long term, and there is no exit strategy– when the patients stop taking the drug, the weight comes back, in addition to the complication associated with it.
- I have also heard that “if it were bad, then the FDA would not approve it.” well, let’s think about it: the FDA approved the Lap band and Phen-Fen, and we all know how these worked out.
- There are no shortcuts, simple injections, or a pill for the complex, multifaceted condition of obesity. Advocating solutions with no long-term outcome, significant complications, and safety concerns is irresponsible.
- A diabetic patient should take the medication LIFELONG to control their blood sugars, including the GLP-1 agonist class of drugs. The concerns are for these medications being used for the treatment of obesity,
SUMMARY: Buyers beware- those who choose to embark on the dangerous load of GLP-1 agonist medications should be prepared to deal with the short and long-term complications of the medication and its withdrawal. This is like the problems that are being seen with patients who choose to have a lap band because it was advocated as simple, reversible, and the Phen fen medication for weight loss with the associated cardiac complication.
https://www.dssurgery.com/wp-content/uploads/2024/09/P000008S017b.pdf
https://www.dssurgery.com/wp-content/uploads/2024/09/20-year-all-procdure-metaanalysis.pdf
https://www.dssurgery.com/weight-loss-injection/
https://www.dssurgery.com/glp-1/
https://www.dssurgery.com/weight-loss-medications-compared-to-surgery/
https://www.dssurgery.com/articles/glp-1-agonists-a…agency-clinicians/
https://www.dssurgery.com/articles/managing-the-gas…clinical-practice/Surgery Bests Lifestyle Changes, GLP-1 for Durable Weight loss
September 11, 2024 9:04 pm
 SAN DIEGO-Bariatric surgery far outperforms lifestyle interventions and glucagon-like peptide-1 (GLP-1) medications at maintaining weight loss, according to a meta-analysis presented at the 2024 annual meeting of the American Society for Metabolic and Bariatric Surgery.
SAN DIEGO-Bariatric surgery far outperforms lifestyle interventions and glucagon-like peptide-1 (GLP-1) medications at maintaining weight loss, according to a meta-analysis presented at the 2024 annual meeting of the American Society for Metabolic and Bariatric Surgery.
With results from six randomized controlled trials, three systematic reviews, and more than 40,000 patients, the study is the first synthesis of its kind.
“The analysis included two systematic reviews of bariatric surgery, one of Roux-en-Y gastric bypass including8,665 patients and one of sleeve gastrectomy including 6,095 patients: a single systematic review or lifestyle interventions including 723 patients; and six randomized controlled trials of GLP-1 medications, including four studies of semaglutide with a total of 11,871 patients and two of tirzepatide with 3,209 patients.
Lifestyle interventions were the least effective treatment, the investigators found, producing a mean total body weight loss of 7.4% at the end of the treatment period, followed by a mean per-month weight regain of 0.14%, with participants reaching their pre-intervention weights within 4.1 years.
GLP-1 medications proved more effective. Weekly semaglutide injections for 20 weeks and tirzepatide for 36 weeks produced a mean total body weight loss of 10.6% and 21.1%, respectively. Roughly half of the weight lost was regained within a year after stopping injections; with continued injections, weight loss plateaued after 17 to 18 months, at 14.9% for semaglutide and 22.5% for tirzepatide.
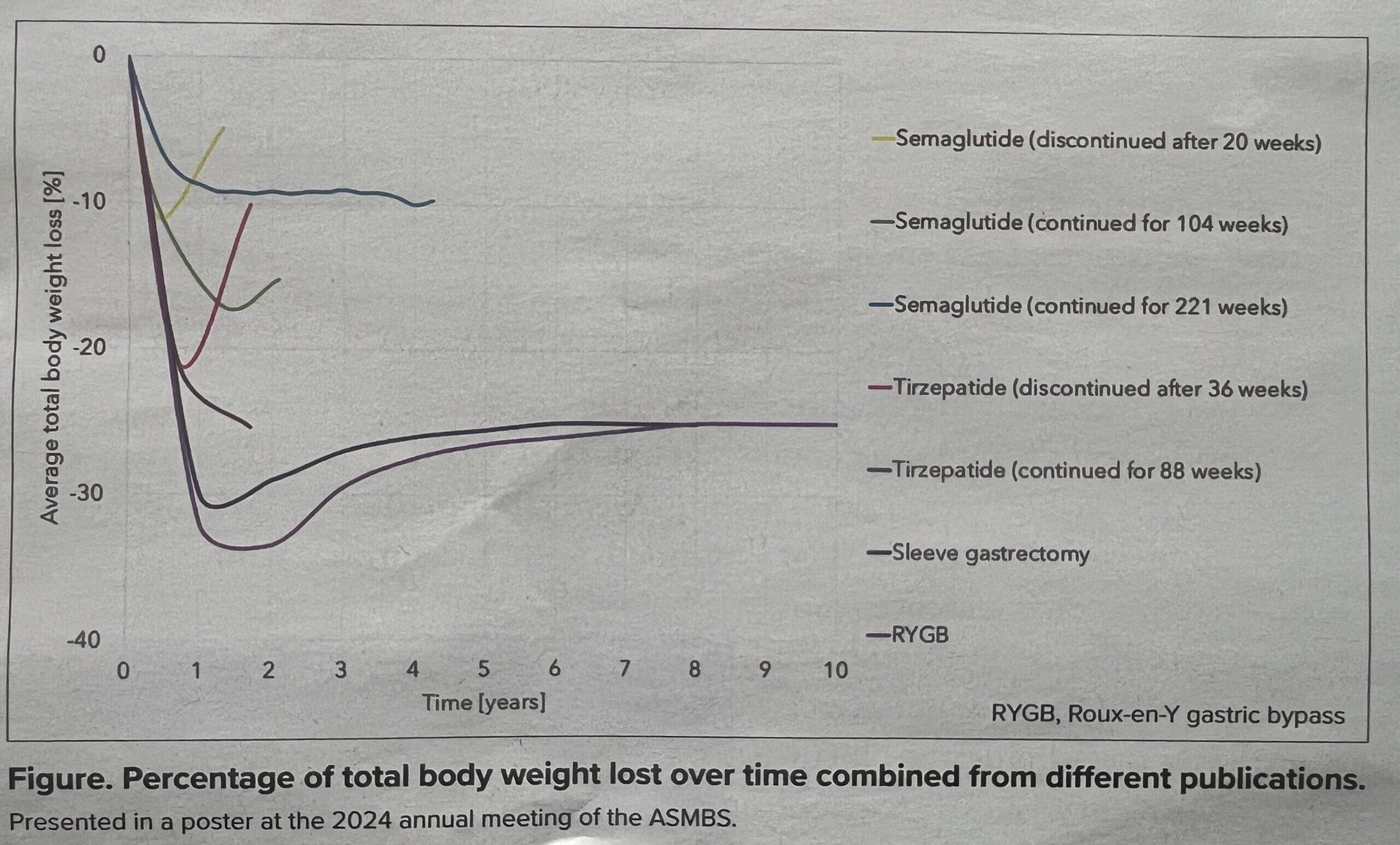
Outcomes after surgery were significantly better. Gastric bypass surgery and sleeve gastrectomy resulted in a mean total body weight loss of 31.9% and 29.5%, respectively, one year after surgery. Accounting for weight regained in the decade after surgery, both procedures produced a stable total body weight loss of approximately 25%.
While the results demonstrate a striking difference favoring surgery, lead investigator Megan Jenkins, MD, a bariatric surgeon at NYU Langone Medical Center in New York City, emphasized that surgery and medication ought to be viewed not in opposition but through a holistic lens as options and potential complements based on the needs of each patient.
“One of the big benefits of these new medications is that it’s helped us to treat obesity as a chronic disease,” Dr. Jenkins said. “We’ve always treated it that way, but I think the medical field has had trouble truly seeing it as a chronic disease. Like diabetes and high blood pressure, for example, which have always been treated with a combination approach.
Sleeve Gastrectomy in Adolescent patients
September 23, 2020 5:44 am
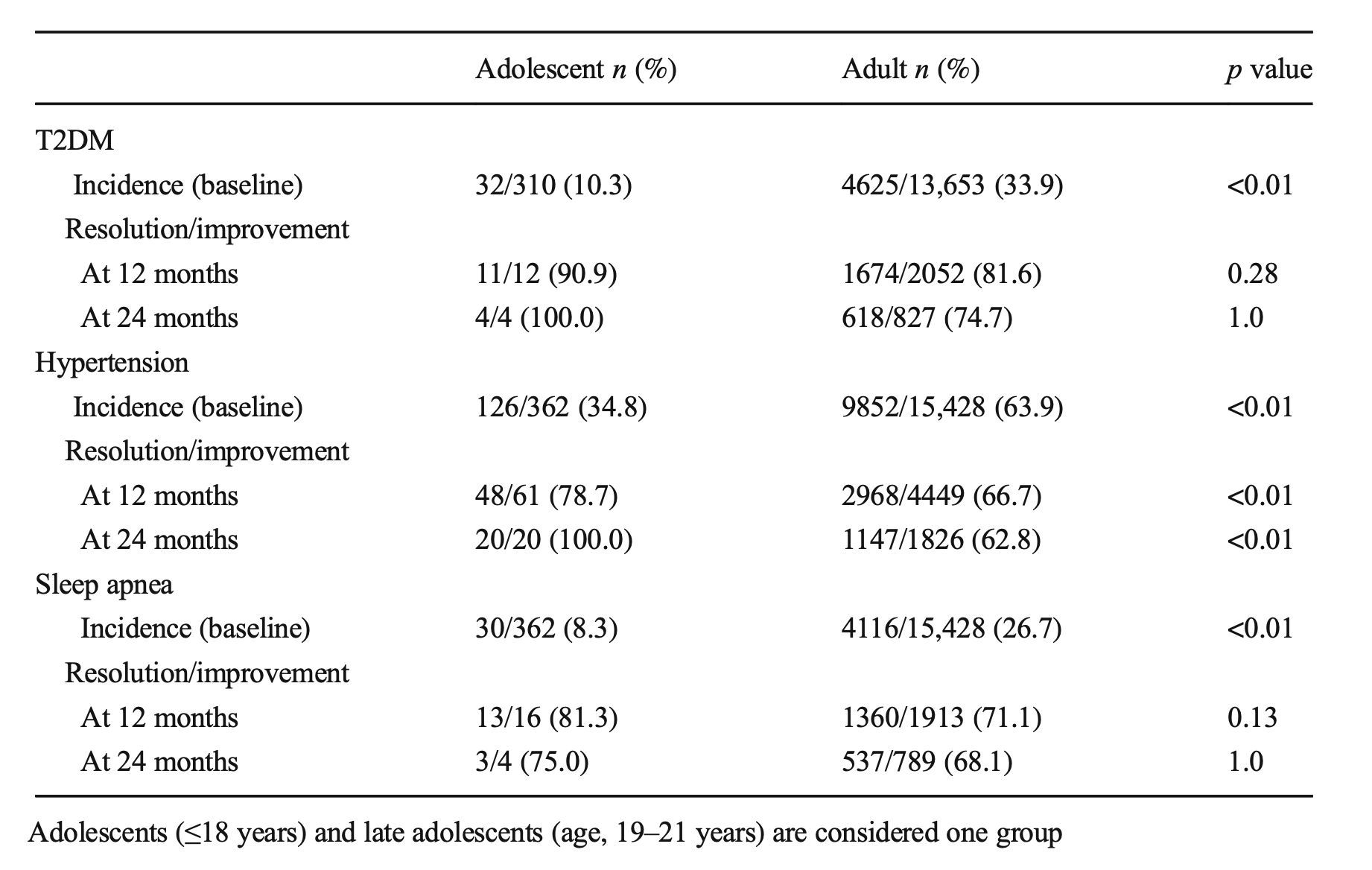 Sleep apnea resolved at the same rate. These early interventions can mean there may be lower long-term risk and associated conditions for these teens as they age.
A recent article was written from several adolescent weight loss surgical patients’ perspectives: This included their feelings of hope for their futures and health.
Sleep apnea resolved at the same rate. These early interventions can mean there may be lower long-term risk and associated conditions for these teens as they age.
A recent article was written from several adolescent weight loss surgical patients’ perspectives: This included their feelings of hope for their futures and health.
Zoom Group Meeting
September 21, 2020 7:10 am
We are excited to announce we will be having a Zoom group meeting Tuesday, September 22, 2020 at 7:00 PM PST. We hope to see you online!
Registration is required. Please follow the link to the meeting registration.
Fat Soluble Vitamins
April 26, 2020 10:20 am
Written By: Maria Vardapetyan, Eric Baghdasaryan, Osheen Abnous
Vitamins are chemicals that facilitate many processes in the human body such as blood clot formation, good vision, fight infections etc. There are two classes of vitamins. Water soluble vitamins and fat soluble vitamins. Water soluble vitamins dissolve in water. This makes it possible for them to be absorbed through all mucous membranes. Fat soluble vitamins on the other hand do not dissolve or pass through mucous membranes. Fat-soluble vitamins are absorbed in the intestine along with fats in the diet. These vitamins have the ability to be stored in the fat tissues of the human body. Water-soluble vitamins are not stored in the body and have to be taken in daily with the food and dietary supplements. Solubility of a vitamin is not a function of its physical state. There are fat soluble vitamins that have a liquid form and almost all of the water soluble vitamins come in form of pills or powders.
In this article, we are going to focus on fat soluble vitamins. They are all complex molecules made of carbon, hydrogen, and oxygen in different arrangements (see figures 1, 2, 3 and 4). These fat soluble vitamins are vitamin A, D, E and K.
Vitamin A
Vitamin A has a major role in vision, immune function, cell growth, and maintenance of organs such as heart, kidneys, lungs, etc. It plays a pivotal role in the health of our eyes, specifically the retina1. Rhodopsin protein, a major protein that has the leading role in the process of vision, is found in the retina where it allows us to perceive light. This protein requires vitamin A to function properly. Without vitamin A, rhodopsin cannot sense light and thus cannot initiate the process by which vision occurs.

Figure 1: Chemical structure of Vitamin A molecule
Vitamin D
Vitamin D regulates different chemical reactions that are associated with bones, muscles, and the immune system. The simplified way it does this regulation is it helps absorb calcium from dietary nutrients which in turn strengthens the bones, helps neurons exchange signals to move muscles and helps the immune system to fight against viruses and bacteria2.
 Figure 2: Chemical structure of Vitamin D molecule
Figure 2: Chemical structure of Vitamin D molecule
Vitamin E
Vitamin E acts as an antioxidant. Antioxidants are naturally occurring chemicals that neutralize toxic byproducts of many chemical reactions in the human body. When food is consumed and digested, the human body converts it into energy. As a result of metabolism free radicals (toxic byproducts) are formed and are neutralized with the help of vitamin E. In addition, free radicals are also in the environment. Furthermore, vitamin E stimulates the immune system to fight against bacteria and viruses3.
 Figure 3: Chemical structure of Vitamin E molecule
Figure 3: Chemical structure of Vitamin E molecule
Vitamin K
Vitamin K can be obtained from food and dietary supplements. There are two forms of vitamin K: phylloquinone (Vitamin K1), which is found in spinach, kale and other greens and menaquinone-4 (Vitamin K2), which is found in animal products. Vitamin K1 is involved in blood clotting, and Vitamin K2 is involved in bone tissue building. Vitamin K1 is the main Vitamin K in human diet (75-90% of all vitamin K consumed), however, it is poorly absorbed in the body4,5.

Figure 4: Chemical structures of Vitamin K1 and K2 molecules
Absorption of fat soluble vitamins
Polarity describes the inherent charge(positive or negative) or lack of charge for any given substance or molecule. Molecules that are charged are referred to as “polar”, while those that lack charge are “nonpolar”. When discussing solubility, it is important to remember the phrase “like dissolves like”. That means polar (charged) substances like to interact with a polar environment like water, since water contains a slight negative charge. Hence, charged substances are water-soluble. Nonpolar substances on the other hand readily interact with nonpolar environments such as fat, which contains no charge. Therefore, molecules that lack a charge such as vitamins A, D, E, and K are referred to as fat soluble.
Due to their water fearing nature, these fat soluble vitamins cannot simply be absorbed directly into the bloodstream (which is mostly water) like the sugars and amino acids in our diet. As their name suggests, these fat soluble vitamins like to be embedded in fatty droplets, which facilitate their absorption in the following way. Fat soluble vitamins group together with other fat molecules to form fatty droplets, effectively reducing the amount of interaction with the watery environment of the intestines. Therefore, without an adequate amount of fat in your diet, your body is unable to effectively absorb these fat-soluble vitamins. This may be true in an intact anatomy, however, post weight loss surgical patients can not increase their fat soluble vitamin levels by increasing their fat intake. This is due to the fact that a high fat diet causes excessive bowel movement which in turn washes away any vitamins taken by mouth. DS limits fat absorption (thus the great weight loss) which can cause vitamin A and D deficiency that can not be easily corrected with oral supplementation.
As mentioned before, fat soluble vitamins are hydrophobic and nonpolar, which means they are also fat loving or lipophilic. Excess fat soluble vitamins can be stored in the liver and fat tissue. Therefore, these vitamins do not need to be eaten every single day since stores of these vitamins can sustain a person for some time. It may take several weeks or months for our body to deplete these stores of fat soluble vitamins which is why it generally takes a longer amount of time for fat soluble vitamin deficiencies to manifest themselves. The ability to store these fat soluble vitamins in tissues can also lead to vitamin toxicity – marked by an excess of vitamin stores in our body.
Clinical manifestations of A, D, E, K deficiency
| Vitamin | Clinical Deficiency manifestations |
| Vitamin A | Vision Problems
Dryness of the eye |
| Vitamin D | Softening and weakening of the bones
Bone shape distortion Bowed legs (generally in children) Hypocalcemia |
| Vitamin E | Damage to red blood cells
Tissue/organ damage due to inability to supply enough blood Vision problems Nervous tissue malfunction |
| Vitamin K1 | Excessive bruising
Increased bleeding time Small blood clots under nails Increased bleeding in mucous membrane |
| Vitamin K2 | Weak bones
Increased plaque deposits along gumline Arterial calcification |
References
- Office of Dietary Supplements – Vitamin A. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/#. Accessed April 26, 2020.
- Office of Dietary Supplements – Vitamin D. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminD-Consumer/. Accessed April 26, 2020.
- Office of Dietary Supplements – Vitamin E. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminE-Consumer/. Accessed April 26, 2020.
- Vitamin K. The Nutrition Source. https://www.hsph.harvard.edu/nutritionsource/vitamin-k/. Published July 2, 2019. Accessed April 26, 2020.
- Beulens JWJ, Booth SL, van den Heuvel EGHM, Stoecklin E, Baka A, Vermeer C. The role of menaquinones (vitamin K₂) in human health. The British journal of nutrition. https://www.ncbi.nlm.nih.gov/pubmed/23590754. Published October 2013. Accessed April 26, 2020.
Diabetes and Weight Loss Surgery
April 06, 2020 5:51 am
The scientific literature is riddled with evidence pointing to the benefit of early metabolic surgery as a superior treatment, remission and possible cure option for diabetes. Unfortunately, the medical education, pharmaceutical companies, primary care healthcare delivery systems and third party payers (health insurance companies) have not caught up with the published data. The American Diabetes Association has changed their guidelines to reflected the benefit for combating diabetes with weight loss surgery.
There is ample evidence of the superior outcome of surgery as a treatment option for diabetes when compared to medical managment. Cummings et.al, in a published article in Diabetes Care, showed sustained stabilization of the Hemoglobin A1C six years after surgery. In contrast, there was no significant changes noted in the non-surgical group.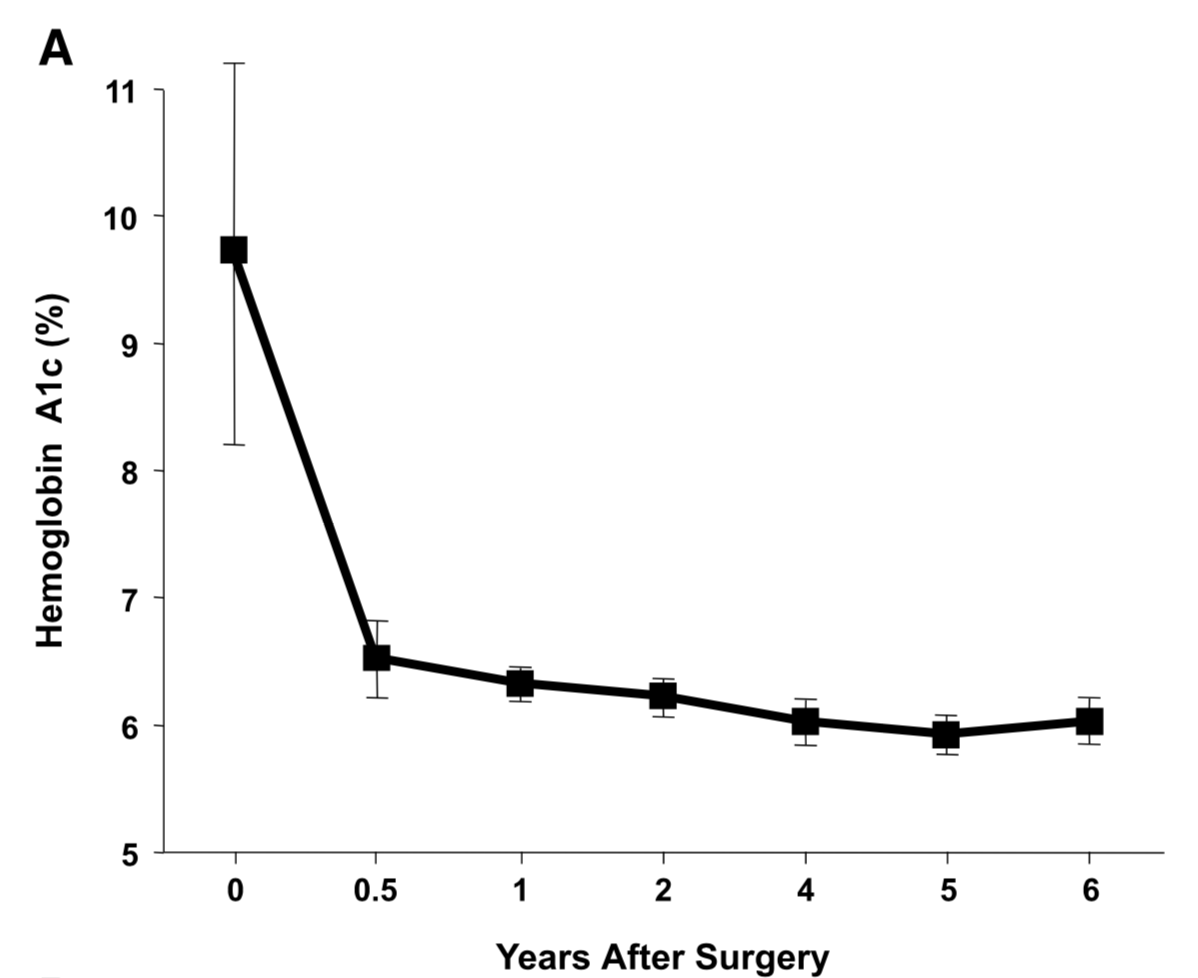
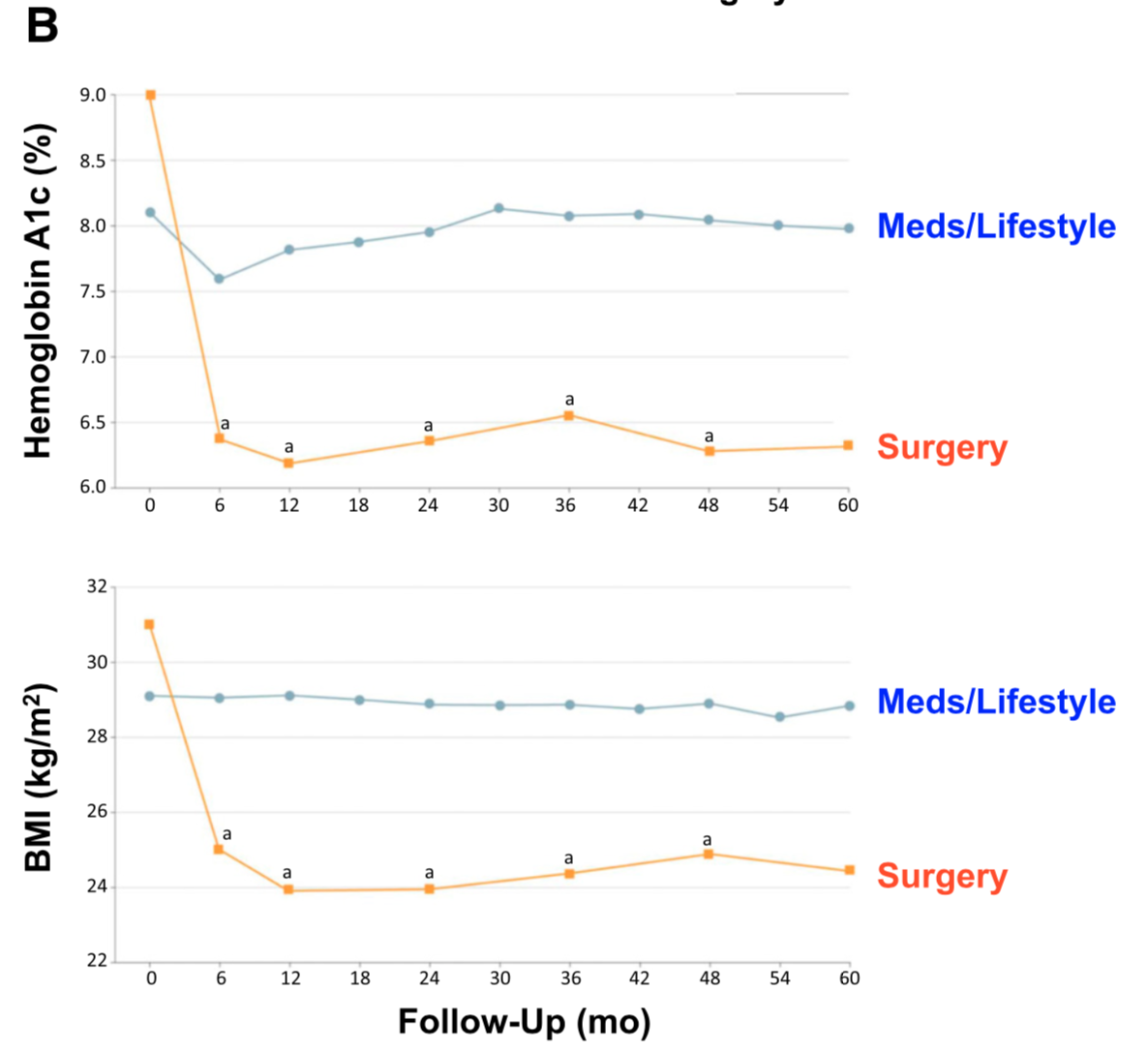
Jans et.al. , in November of 2019 showed that the patients who had NOT been on Insulin, and had metabolic surgery had the highest long term success for resolution and remission of the diabetes. This identifies that having a patient be proactive in their care by having metabolic surgery improves success rates.
The exact mechanism by which the diabetes is resolved is unclear. The weight loss may play a role. There are numerous hormones and neuroendocrine modulators which control the complex metabolic pathways. Batterham et.al., in Diabetes Care (2016), published a summary overview of the possible mechanism involved in diabetes improvement following metabolic surgery.

There are a number of overlapping and sequential layers for possible reasons why diabetes resolves after weight loss/metabolic surgery. These may be directly related to surgery and the reduction of the calorie intake or absorption. It may also involve the neuroendocrine modulators.
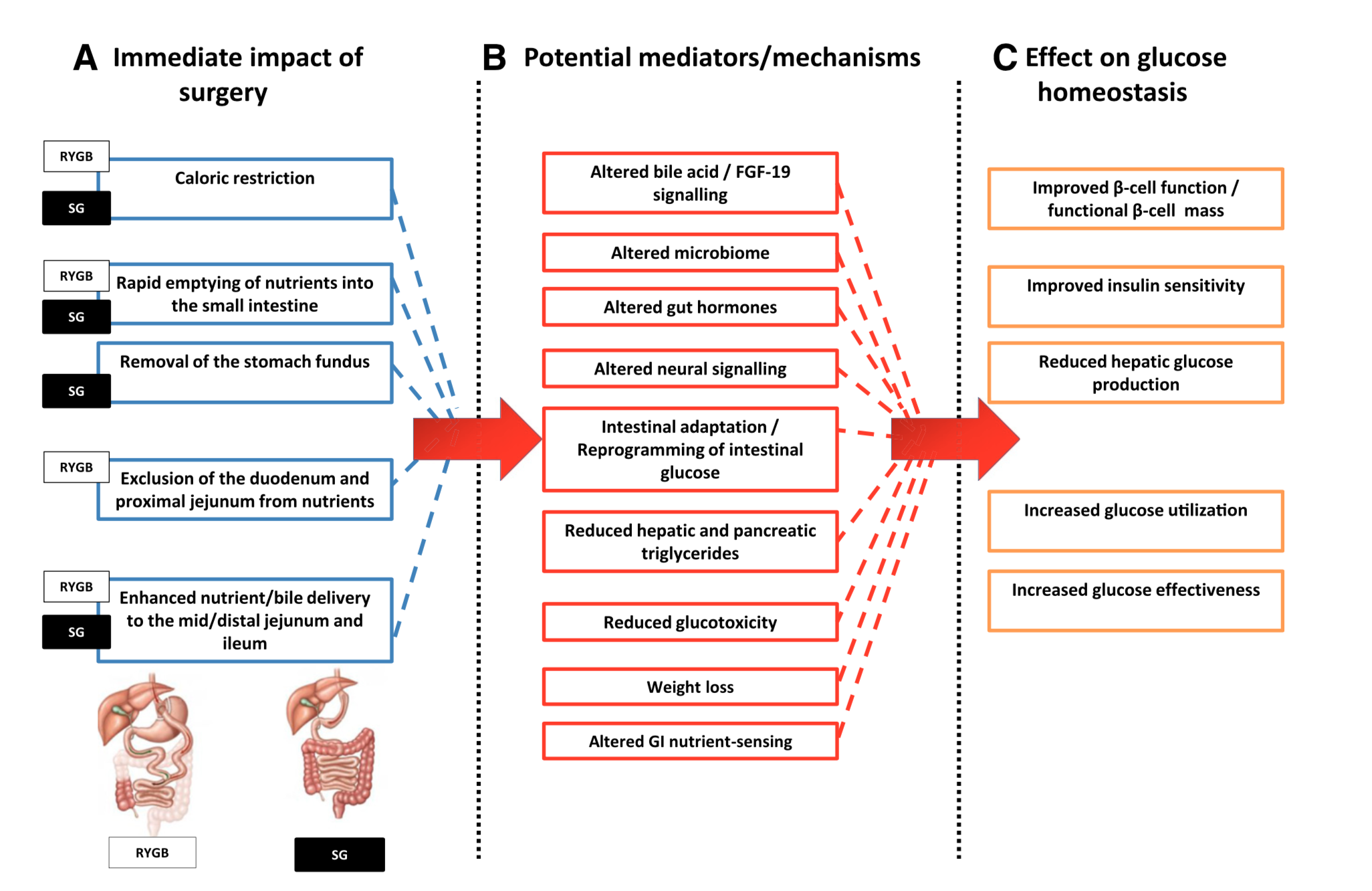
What can be said definitively is that early surgical intervention is best and most likely the only permanent solution to type II diabetic resolution. There is no medical justification in not considering metabolic surgery in diabetic patients who may also have difficulty with meaning a BMI< 35.
Medication Absorption After Weight Loss Surgery
March 30, 2020 8:01 am
Weight loss surgical procedures, in one form or another, achieve the desired effect of weight loss by altering absorption of fat, protein, and carbohydrates. This results in decreased total absorption of required calories.
An unintended consequence is the altered absorption of medications. Frequently I am asked about the specific medication. Usually the answer is vague since the information is limited on specific medications. If the desired effect is not achieved, then it is probably not being absorbed well. Specially, if the same dose of the same medication working well before surgery.
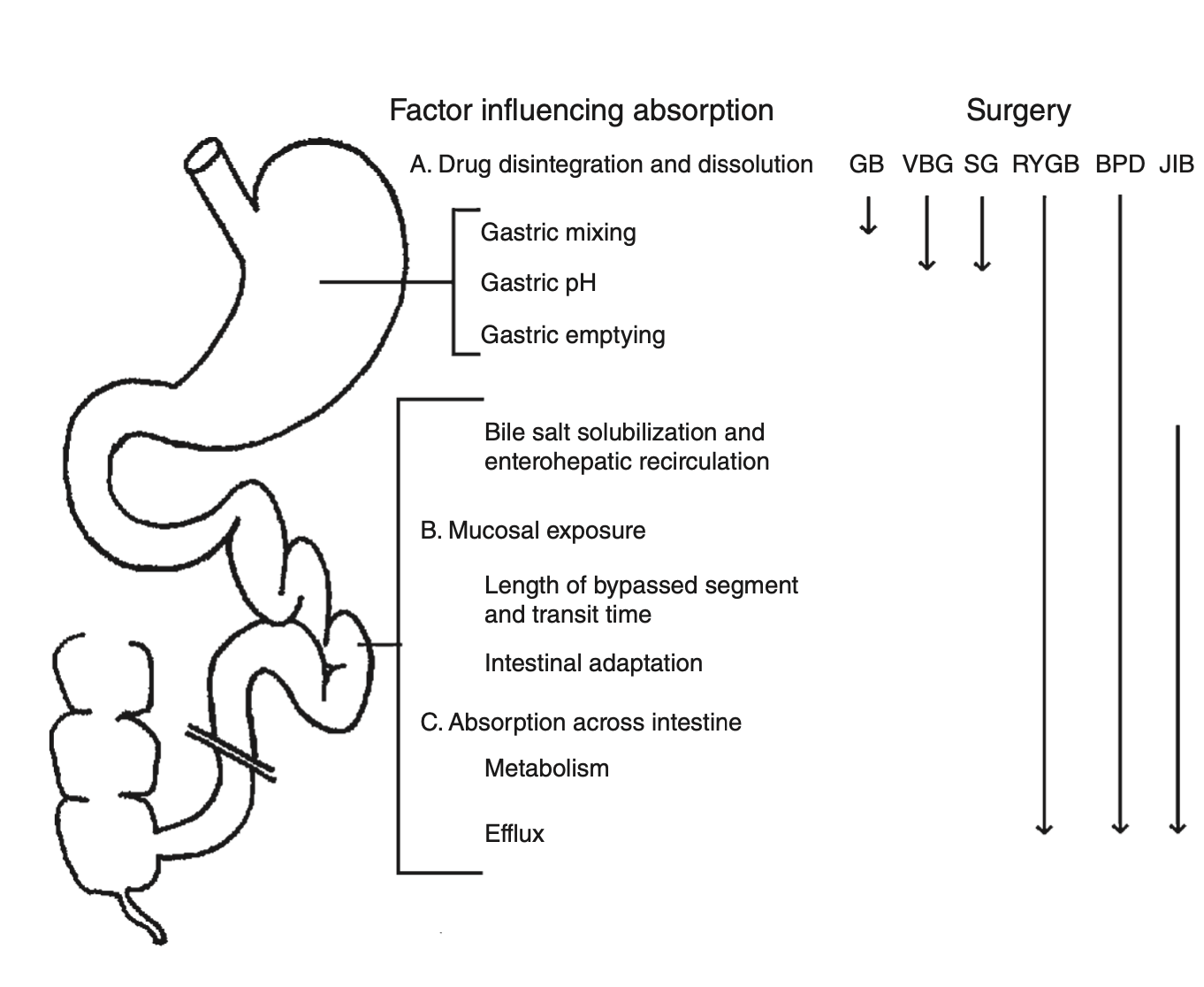
There is a summary article about the Theoretical absorption pattern of different weight loss surgical procedures.
Articles
March 22, 2020 6:57 pm
Sleeve And Weight Regain
July 22, 2019 9:50 am
 Felsernreich et.al. demonstrated that 10 years after sleeve gastrectomy 33% were requiring revisions of their sleeve due to weight regain or reflux. 66% needed revision for weight loss and only 34% for reflux. Those patients who have revision to gastric bypass (in their practice all being revised with two exception) had resolution of their reflux however had no sustained weight loss after the revisions. This supports our position that we have had for years that the those patient who had the sleeve and are experiencing weight regain, recurrence of comorbidities inadequate weight loss ahould all be revised to the duodenal switch operation.
Felsernreich et.al. demonstrated that 10 years after sleeve gastrectomy 33% were requiring revisions of their sleeve due to weight regain or reflux. 66% needed revision for weight loss and only 34% for reflux. Those patients who have revision to gastric bypass (in their practice all being revised with two exception) had resolution of their reflux however had no sustained weight loss after the revisions. This supports our position that we have had for years that the those patient who had the sleeve and are experiencing weight regain, recurrence of comorbidities inadequate weight loss ahould all be revised to the duodenal switch operation. 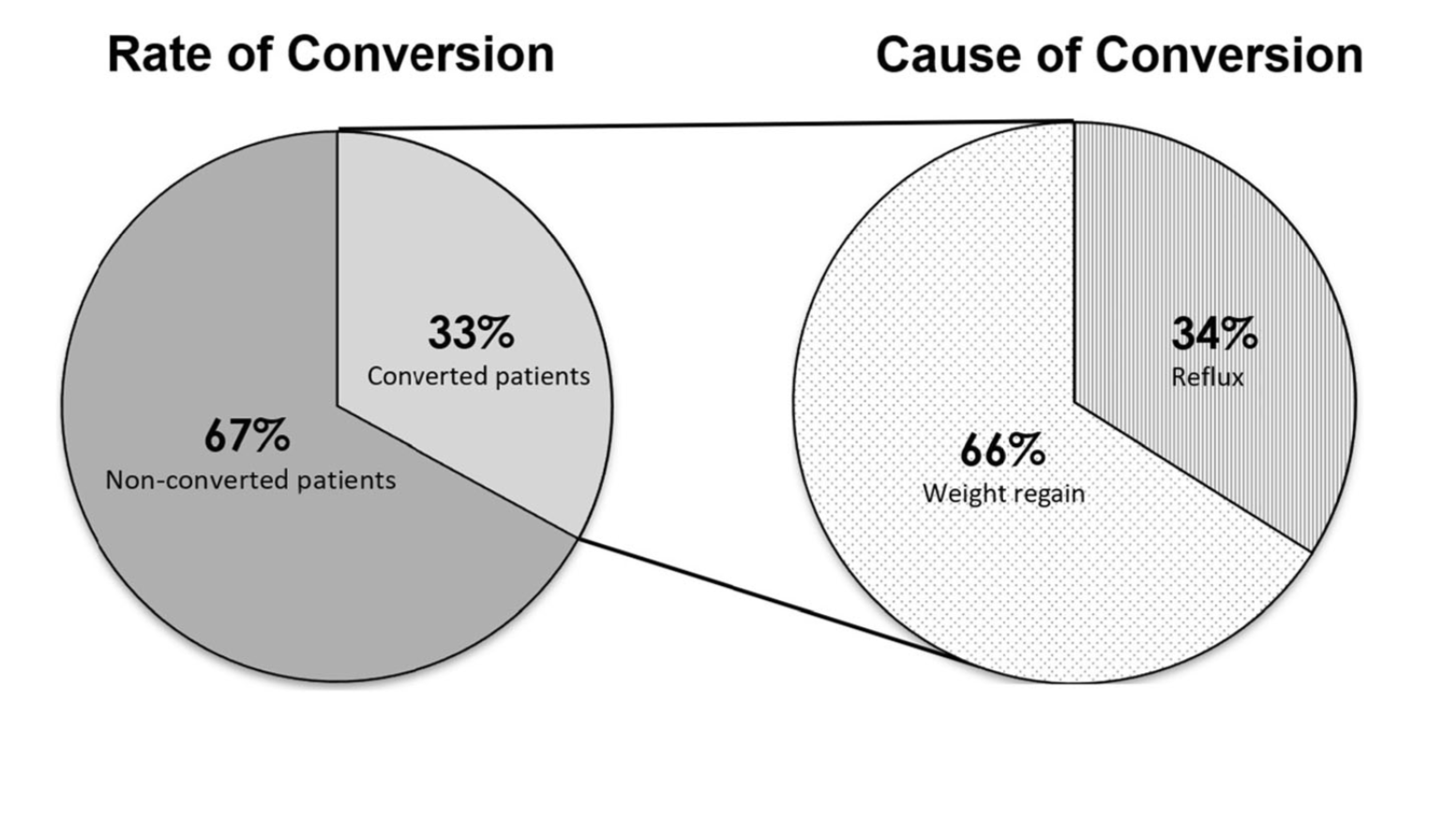
Sunscreen
June 27, 2019 3:03 am
Recently there has been some research and concern regarding sunscreen and the chemicals within them. This has led to findings that can be concerning but that need further research.
Post weight loss surgical patients, and in general patients who suffer with obesity, before or after weight loss surgery, have low vitamin D level. This may be caused by a number of factors. One such factor may be the reluctance to get skin exposed to sunlight in order for the bodies natural Vitamin D pathways functioning.
The recommendations are for daily exposure to sun. This not only is critical to the vitamin D metabolic pathways, but also help with bone health, immune function, mood, counteracting depression.
In a recently published online article, concerns were raised that some of the ingredients of some of few sunscreens are absorbed in the blood stream. This is a small study, and as the results indicates, it is not recommending to stop using the sun screens. Be aware of your sun exposure, timing exposure, and the ingredients in your sunscreen.
You can find past blog posts on Vitamin D, Bone health, etc here