
Tag: Duodenal Switch
Vitamin Toxicity
December 17, 2024 1:36 pm
Patients are frequently asked to explain why they take high fat- or water-soluble vitamin doses. They are have often been scared by their well meaning healthcare providers that their higher levels of vitamin supplements will end up with vitamin toxicity.
Let’s clarify one point: there is such a thing as too much vitamin.
However, the point that is often overlooked in teaching within professional schools (medical, nursing, pharmacy, etc.) and drug manufacturers is that recommendations are based on “how much to take” and not how much is needed to keep a patient’s blood level in the normal range.

This table highlights how toxicity is described and what requirements are recommended. Vitamin toxicity is seen rarely in post-weight loss surgical patients who take them proactively in as many doses as needed to get their blood levels in the normal range. I see more patients in the office who suffer from low vitamin levels, such as vitamin D and A levels (duodenal switch and sleeve), than any patient with high or toxic levels of any vitamins.
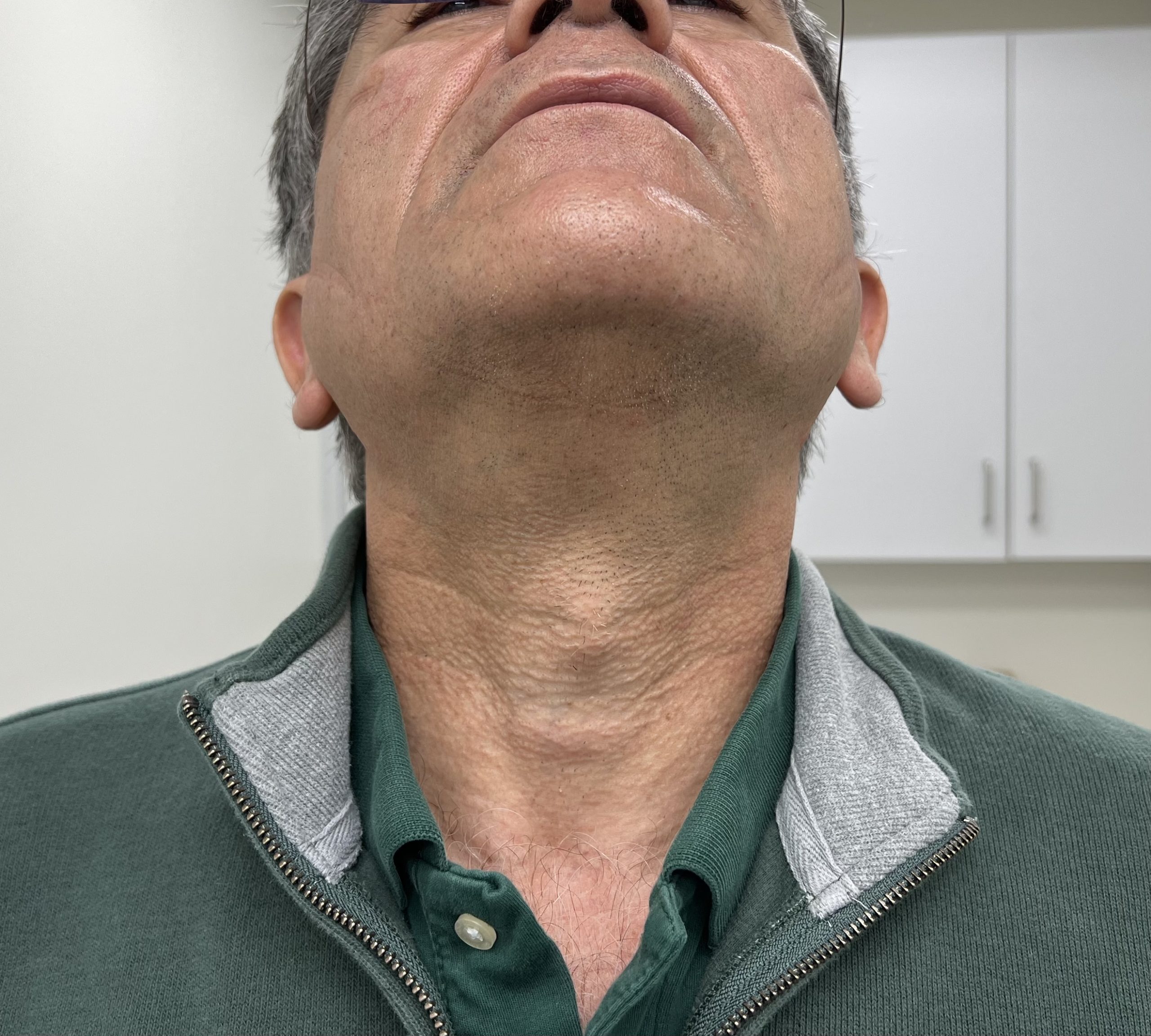
Here is an example of critical vitamin A deficiency and night blindness and how, with aggressive large-dose supplementation, her condition was corrected.
A patient story: Lap Band complication and Wegovy
October 24, 2024 4:30 pm
Not too long ago, I saw an old patient who had seen me years ago after having had a lap band placed for weight loss. At the time, I recommended that the lap band be removed and that alternative plans be made. I suspected a slipped band. We discussed the reality that after the band removal, weight gain is to be expected. Several surgical options were discussed, and the patient dismissed them as “too radical.” The patient decided to “deal” with the ongoing nausea and vomiting since it was a small price to pay for the weight loss. I warned the patient that elective removal of the band is much safer than an emergency procedure in the middle of the night when it is least convenient. The patient did end up with an emergency lap band removal and was started on GLP-1 Agonists (Wegovy) because of the weight gain that followed the band removal. The side effects of the medication were debilitating, with nausea, dizziness, and fainting due to low blood sugar. The drug has all been stopped, and most, not all, of the side effects are resolved. The plan is to get this patient in a better shape and, reevaluate the esophagus and the stomach, and formulate a strategy based on the blood work, upper endoscopy, upper GI study findings and decide if the patient will be a good candidate for the Laparoscopic sleeve or the duodenal switch operation.
Here are my recommendations:
- Patients should avoid lap bands. Those with lap bands, regardless of how they feel and whether they are having issues with them, should have the lap band removed immediately before they end up in the emergency room or have irreversible changes to the cells or function of the stomach and esophagus.
- Patients who have the lap band removed will have less weight loss with the sleeve than those who have the sleeve as the primary procedure (the lesson here is that a less invasive, seemingly easy solution is much worse long term; more on this below). Lap Band patients should be revised to the duodenal switch, SPIS, SADI, or Gastric bypass if they have substantial weight to lose.
- GLP-1 agonist medication should be avoided. It is not a solution to the underlying problem but a band-aid covering the metabolic derangement.
- GLP-1 agonist medication needs to be taken long term, and there is no exit strategy– when the patients stop taking the drug, the weight comes back, in addition to the complication associated with it.
- I have also heard that “if it were bad, then the FDA would not approve it.” well, let’s think about it: the FDA approved the Lap band and Phen-Fen, and we all know how these worked out.
- There are no shortcuts, simple injections, or a pill for the complex, multifaceted condition of obesity. Advocating solutions with no long-term outcome, significant complications, and safety concerns is irresponsible.
- A diabetic patient should take the medication LIFELONG to control their blood sugars, including the GLP-1 agonist class of drugs. The concerns are for these medications being used for the treatment of obesity

Radiology film of normal position and a slipped LapBand
SUMMARY: Buyers beware- those who choose to embark on the dangerous load of GLP-1 agonist medications should be prepared to deal with the short and long-term complications of the medication and its withdrawal. This is like the problems that are being seen with patients who choose to have a lap band because it was advocated as simple, reversible, and the Phen fen medication for weight loss with the associated cardiac complication.
https://www.dssurgery.com/wp-content/uploads/2024/09/P000008S017b.pdf
https://www.dssurgery.com/wp-content/uploads/2024/09/20-year-all-procdure-metaanalysis.pdf
https://www.dssurgery.com/weight-loss-injection/
https://www.dssurgery.com/glp-1/
https://www.dssurgery.com/weight-loss-medications-compared-to-surgery/
https://www.dssurgery.com/articles/glp-1-agonists-a…agency-clinicians/
https://www.dssurgery.com/articles/managing-the-gas…clinical-practice/Should Adjustable Gastric Banding (Lap Band) be done?
October 06, 2024 9:17 pm
 The Lap Band was approved in the US in 2001 (BMI> 40). The following studies used only small samples and examined short-term efficacy and safety. They were then performed to consider the utility of the Laob band for patients with lower BMI (BMI 30-40).
The Lap Band was approved in the US in 2001 (BMI> 40). The following studies used only small samples and examined short-term efficacy and safety. They were then performed to consider the utility of the Laob band for patients with lower BMI (BMI 30-40).  Noe the frequent complications of nausea, difficulty swallowing, pain, and reflux-which may sound familiar to a lot of patients who have had and still have the Lap Band.
Numerous US and international studies have been published over the years, including short-term and long-term studies. The summary outcome has been the same, with only a few exceptions.
Noe the frequent complications of nausea, difficulty swallowing, pain, and reflux-which may sound familiar to a lot of patients who have had and still have the Lap Band.
Numerous US and international studies have been published over the years, including short-term and long-term studies. The summary outcome has been the same, with only a few exceptions.
- The Lap Band does not result in long-term sustained weight loss.
- Lap band has significant complications, some of which may not be reversible.
- The lap band can be removed, but eroding the banc to the stomach is not easy.

Bile Reflux Gastritis
August 02, 2024 10:53 am
Bile Reflux
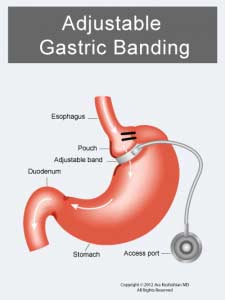
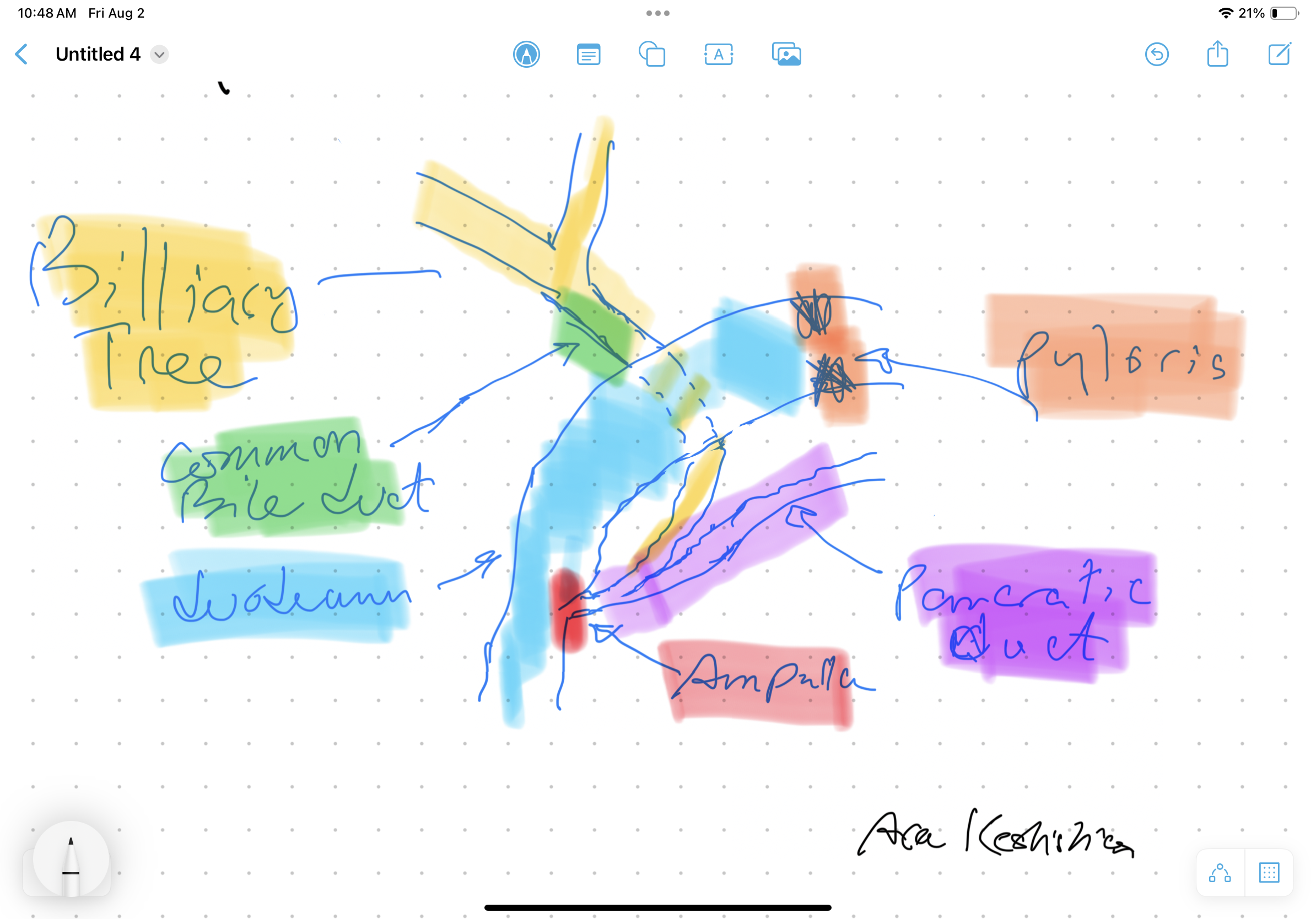
Bile Reflux is primarily a diagnosis of exclusion. All other possible causes must be ruled out, and bile reflux gastritis is made with the pertinent symptoms. The reason for this is that there is no primary test that can prove the diagnosis. When it comes to treatment, the surgical option requires preventing the bile from coming back to the stomach. The procedure we have performed routinely for bile reflux gastritis is the duodenal switch (without a reduction in the stomach size). This allows the food to go through an intact stomach and pyloric valve with normal stomach physiology (to prevent dumping syndrome). The bile is diverted through 100 cm of the small bowel as the biliary and alimentary limbs to prevent backflow of bile to the stomach (if it’s made too short). The procedure referenced (https://www.americanjournalofsurgery.com/article/S0002-9610(03)00213-7/abstract) is nearly 20 years old. It is rarely, if at all, performed due to its very complex and relatively high-risk nature. Its primary role for a surgeon is to reconstruct the biliary track flow. This operation involved transecting the common bile duct and creating a biliary tree to small bowel anastomosis. This is, at times, done when there is injury, obstruction, or tumor of the bile duct. This anastomosis has its complications, including stricture and sump syndrome. Therefore, hepaticojejunostomy or hepato-duodenostomy anastomosis are reserved for cases with no alternatives. A-Normal Anatomy
B-Duodenal switch for bile Reflux
C-Hepatojejunostomy for bile relaxation was proposed in a 2003 study.
A-Normal Anatomy
B-Duodenal switch for bile Reflux
C-Hepatojejunostomy for bile relaxation was proposed in a 2003 study.

SIPS-SADI and ASMBS
December 31, 2023 1:21 pm
Pictures For Anesthesia
February 02, 2022 11:57 am

Covid 19:Anesthesia, Weight Loss Surgery and Malnutrition
October 30, 2021 8:52 am
As the COVID-19 pandemic is charting its course into 2022, as health care providers, we have had to adapt and adjust to the transient and shifting environment. Testing for COVID-19 has been in place, and is now part of the standard for preoperative work-up. In addition, covid testing will likely be part of screening any surgical procedure for the foreseeable future.
The challenge of pandemic control is the large pockets of populations in the US and worldwide that do not have protection against the virus and are not vaccinated. Vaccination provides the only proven long-term protection against COVID-19 infection and its long-term persistent health effect. In addition, the complication rate reported in scientific journals is negligible compared to the complication and death rate from the COVID-19 infection.
There are implications of covid infection and general anesthesia published in peer-reviewed journals. The increased risk of general anesthesia after covid infection is related to the severity of the initial infection and the extent of the treatment required, and the persistence of the post covid symptoms, including shortness of breath, fatigue, and laboratory finding elevated inflammatory markers. Long after resolution of the acute COVID-19 symptoms, the most common persistent complaints are fatigue, shortness of breath, Joint and chest pain; and all these increase the risk of post-operative complications (Carfì et al., 2020)
The required delay for surgery may be as short as 2-4 weeks to as long as six months or longer if the persistent symptoms are present. Surgery may not be avoidable in a critical life-threatening situation and may be necessary even with a much-increased risk of complication (Collaborative, 2020). Recovery post-COVID-19 may not be complete with the resolution of the initial symptoms (Dexter et al., 2020)
Recent publications and scientific presentations have also shown the protection that weight loss surgery and maintained weight loss provide in those who come down with the COVID-19 infection (Aminian et al., 2021). However, the rate of weight gain, lack of weight loss is worse for weight loss surgical patients post COVID-19 disorder (Bullard et al., 2021; Conceição et al., 2021). Furthermore, patients with COVID-19 infection post weight loss are at a higher risk of malnutrition (di Filippo et al., 2021; Kikutani et al., 2021). Up to 40% of patients have malnutrition if hospitalized with COVID (Anker et al., 2021).
To summarize, Weight loss and weight loss surgery reduce the severity of the initial COVID-19 infection. However, it increases malnutrition risk, requiring nutritional support and surgical interventions in non-responsive cases.
REFERENCES:
Aminian, A., Fathalizadeh, A., Tu, C., Butsch, W. S., Pantalone, K. M., Griebeler, M. L., Kashyap, S. R., Rosenthal, R. J., Burguera, B., & Nissen, S. E. (2021). Association of prior metabolic and bariatric surgery with severity of coronavirus disease 2019 (COVID-19) in patients with obesity. Surgery for Obesity and Related Diseases, 17(1). https://doi.org/10.1016/j.soard.2020.10.026
Bullard, T., Medcalf, A., Rethorst, C., & Foster, G. D. (2021). Impact of the COVID-19 pandemic on initial weight loss in a digital weight management program: A natural experiment. Obesity, 29(9). https://doi.org/10.1002/oby.23233
Conceição, E., de Lourdes, M., Ramalho, S., Félix, S., Pinto-Bastos, A., & Vaz, A. R. (2021). Eating behaviors and weight outcomes in bariatric surgery patients amidst COVID-19. Surgery for Obesity and Related Diseases, 17(6).
Di Filippo, L., De Lorenzo, R., D’Amico, M., Sofia, V., Roveri, L., Mele, R., Saibene, A., Rovere-Querini, P., & Conte, C. (2021). COVID-19 is associated with clinically significant weight loss and risk of malnutrition, independent of hospitalisation: A post-hoc analysis of a prospective cohort study. Clinical Nutrition, 40(4). https://doi.org/10.1016/j.clnu.2020.10.043
Kikutani, T., Ichikawa, Y., Kitazume, E., Mizukoshi, A., Tohara, T., Takahashi, N., Tamura, F., Matsutani, M., Onishi, J., & Makino, E. (2021). COVID-19 infection-related weight loss decreases eating/swallowing function in schizophrenic patients. Nutrients, 13(4). https://doi.org/10.3390/nu13041113
COVID Vaccines
March 05, 2021 3:50 pm
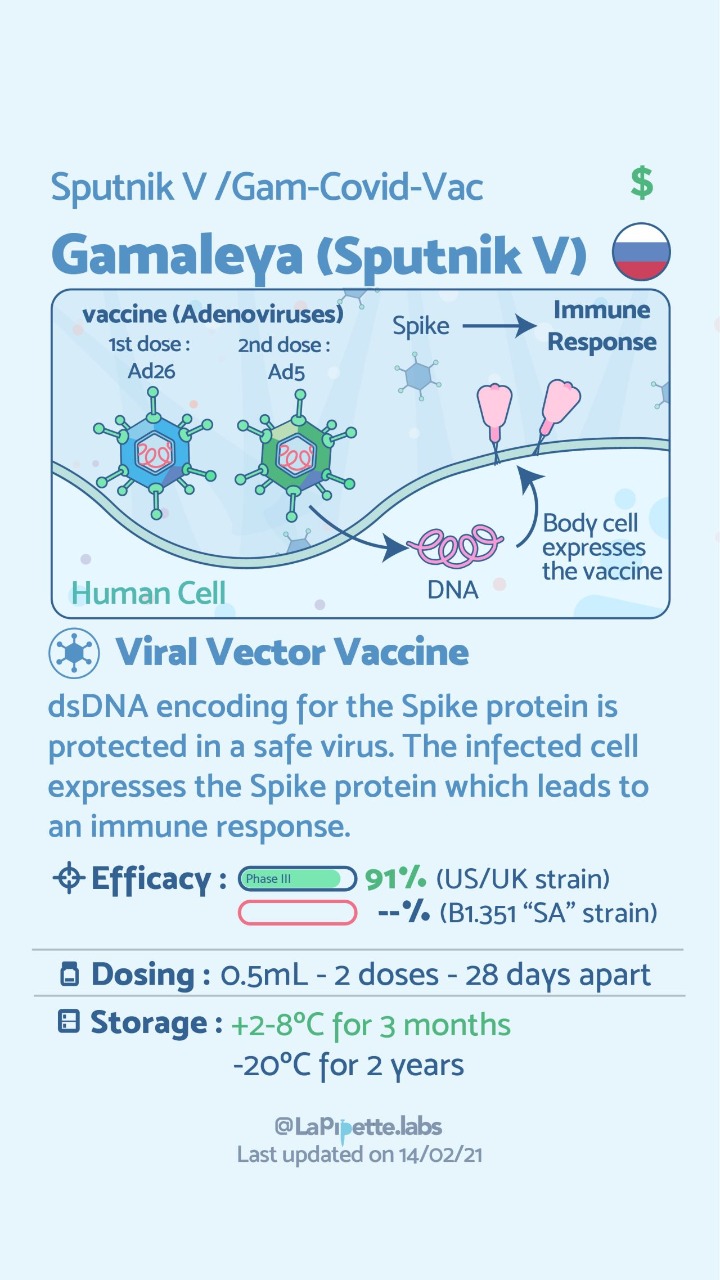
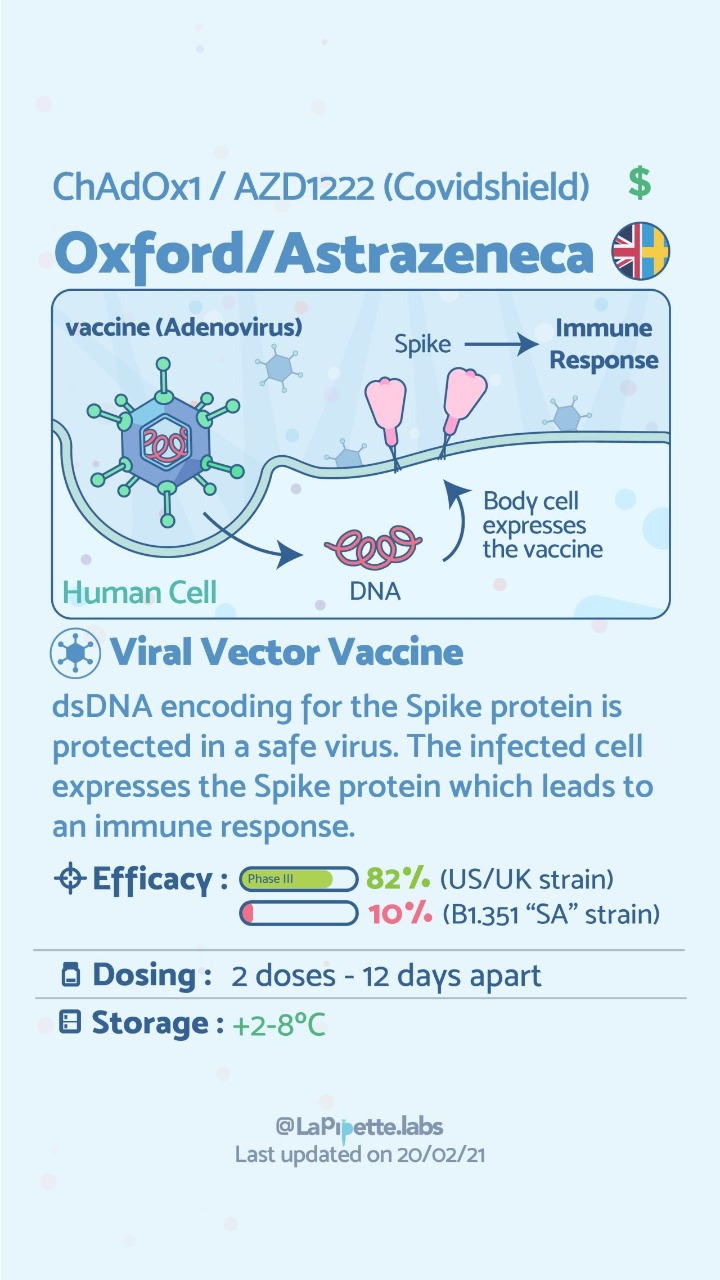
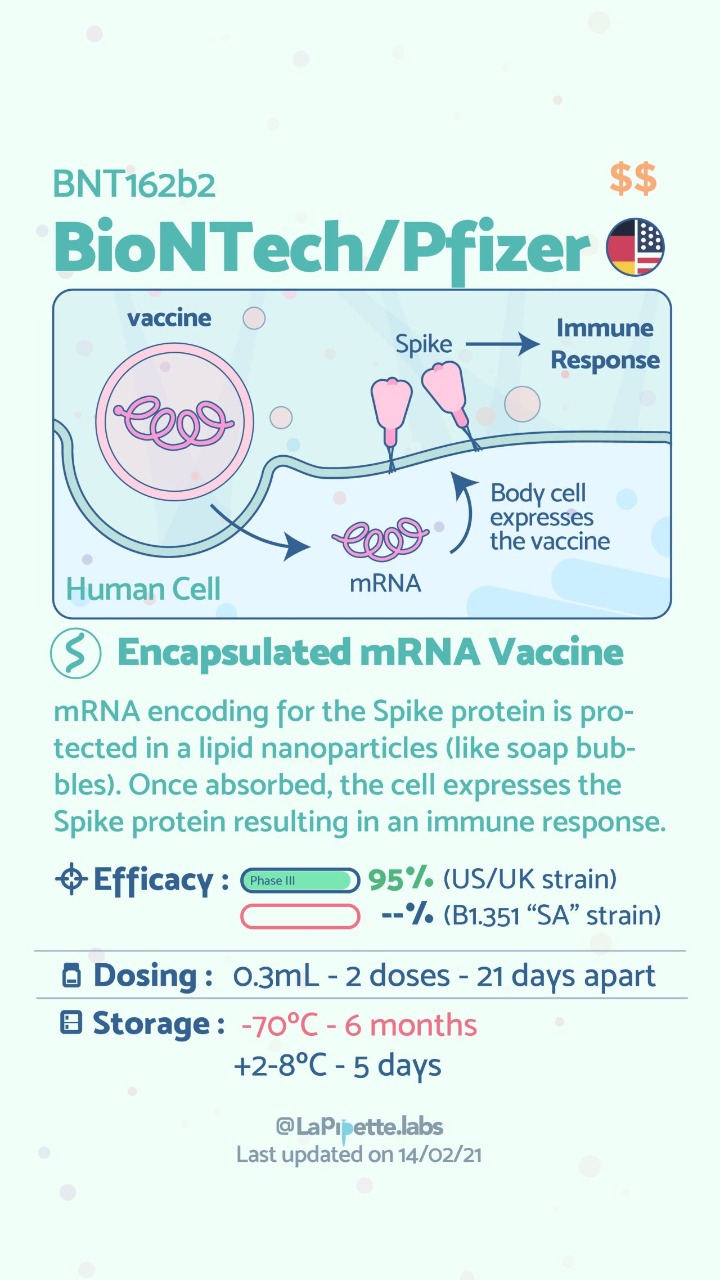
There are no known contraindications from a weight-loss surgical perspective to prevent a post-surgical patient from getting the COVID vaccines.
A patient who has had a Duodenal Switch, Lap Sleeve Gastrectomy, RNY Gastric Bypass, or revisions to Weight Loss Surgery should have the COVID vaccine. The vaccination should be avoided for a few weeks after surgery. For other possible contraindications, please consult your PCP.
Here is a summary of the vaccines and the details of each one approved as of the publication date.



Physical Activity in US
November 28, 2020 1:41 pm
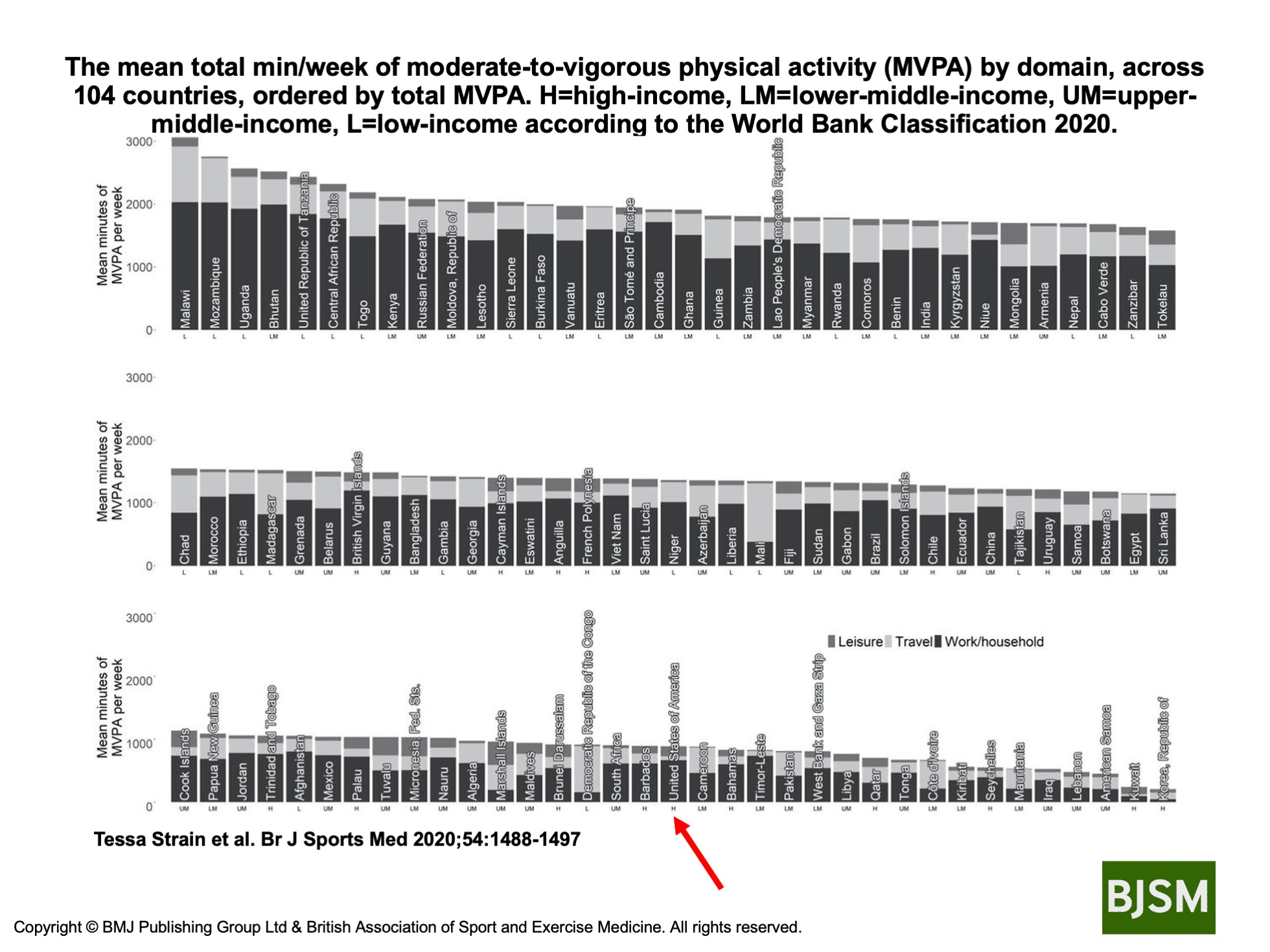
Physical activity in the U.S. varies based on geographic location, socioeconomic status and in comparison to other countries. It is important to know that physical activity is an important component of our well-being. However, this does not mean that going to the gym is the only way to be physically active.
Strain et al. Shows that different populations in different countries get their activity from different sources.
His research showed that the United States population ranked as a high-income country, ranks in the lower 1/3 of the number of countries surveyed with regards to the meeting minutes of moderate-to-vigorous physical activity (MVPA) per week. This may be a contributing factor to the significant rise in obesity in the United States. Individually we should all aim to increase our moderate to vigorous activity significantly.
Activity And Your Health
November 28, 2020 1:26 pm
We should be aware that being physically active is part of being healthy. Health is a combination of being physically active, having a healthy diet are all parts of the variables that contribute to our physical and mental well-being long-term.
The restrictions and the stressors caused by COVID-19 have resulted in our inability to maintain a healthy diet and be physically active. However, we must be vigilant with maintain our activity levels to combat health issues.
It is timely that the British Medical Journal has just published an entire issue regarding the significance of activity and our health as individuals and public health worldwide.
There are a few articles that are outlined here.
Ekelund et al. Reviewed published articles and correlated the activity level and mortality. They Concluded, “Higher sedentary time is associated with higher mortality in less active individuals when measured by accelerometry. About 30–40 min of MVPA per day attenuate the association between sedentary time and risk of death, which is lower than previous estimates from self-reported data.”