
Tag: COVID
Elective Surgery and Anesthesia for Patients after COVID-19 Infection
January 23, 2022 6:03 pm
![]()
![]()
ASA and APSF Joint Statement on Elective Surgery and Anesthesia for Patients after COVID-19 Infection is also available for download (PDF)
Since hospitals are able to continue to perform elective surgeries while the COVID-19 pandemic continues, determining the optimal timing of procedures for patients who have recovered from COVID-19 infection and the appropriate level of preoperative evaluation are challenging given the current lack of evidence or precedent. The following guidance is intended to aid hospitals, surgeons, anesthesiologists, and proceduralists in evaluating and scheduling these patients. It is subject to change as new evidence emerges.
In general, all non-urgent procedures should be delayed until the patient has met criteria for discontinuing isolation and COVID-19 transmission precautions and has entered the recovery phase. Elective surgeries should be performed for patients who have recovered from COVID-19 infection only when the anesthesiologist and surgeon or proceduralist agree jointly to proceed.
What determines when a patient confirmed to have COVID-19 is no longer infectious?
The Centers for Disease Control and Prevention (CDC) provides guidance for physicians to decide when transmission-based precautions (e.g., isolation, use of personal protective equipment and engineering controls) may be discontinued for hospitalized patients or home isolation may be discontinued for outpatients.
Patients infected with SARS-CoV-2, as confirmed by reverse transcriptase-polymerase chain reaction (RT-PCR) testing of respiratory secretions, may be asymptomatic or symptomatic. Symptomatic patients may be further sub-classified into two groups depending upon symptom severity. Table 1 provides definitions of these COVID-related illness levels of severity.
- Patients with mild to moderate symptoms* (generally those without viral pneumonia or oxygen saturation below 94 percent)
- Patients who experienced severe or critical illness** due to COVID-19 (e.g., pneumonia, hypoxemic respiratory failure, septic shock).
Severely immunocompromised patients***, whether suffering from asymptomatic or symptomatic COVID-19, are considered separately.
Current data indicate that, in patients with mild to moderate COVID-19, repeat RT-PCR testing may detect SARS-CoV-2 RNA for a prolonged period after symptoms first appear. However, in these patients, replication-competent virus has not been recovered after 10 days have elapsed following symptom onset. Considering this information, the CDC recommends that physicians use a time- and symptom-based strategy to decide when patients with COVID-19 are no longer infectious.
For patients with confirmed COVID-19 infection who are not severely immunocompromised and experience mild to moderate symptoms*, the CDC recommends discontinuing isolation and other transmission-based precautions when:
- At least 10 days have passed since symptoms first appeared.
- At least 24 hours have passed since last fever without the use of fever-reducing medications.
- Symptoms (e.g., cough, shortness of breath) have improved.
For patients who are not severely immunocompromised and have been asymptomatic throughout their infection, isolation and other transmission-based precautions may be discontinued when at least 10 days have passed since the date of their first positive viral diagnostic test.
In approximately 95 percent of severely or critically ill patients (including some with severe immunocompromise), replication-competent virus was not present after 15 days following the onset of symptoms. Replication-competent virus was not detected in any severely or critically ill patient beyond 20 days after symptom onset.
Therefore, in patients with severe to critical illness** or who are severely immunocompromised***, the CDC recommends discontinuing isolation and other transmission-based precautions when:
- At least 10 days and up to 20 days have passed since symptoms first appeared.
- At least 24 hours have passed since the last fever without the use of fever-reducing medications.
- Symptoms (e.g., cough, shortness of breath) have improved.
Consultation with infection control experts is strongly advised prior to discontinuing precautions for this group of patients. Clinical judgment ultimately prevails when deciding whether a patient remains infectious. Maintaining transmission-based precautions and repeat RT-PCR testing may be appropriate if clinical suspicion of ongoing infection exists. The utility of repeat RT-PCR testing after improvement in symptoms is unknown as patients will frequently remain at least intermittently positive for weeks to months.
If a patient suspected of having SARS-CoV-2 infection is never tested, the decision to discontinue transmission-based precautions can be made using the symptom-based strategy described above.
Other factors, such as advanced age, diabetes mellitus, or end-stage renal disease, may pose a much lower degree of immunocompromise; their effect upon the duration of infectivity for a given patient is not known.
Ultimately, the degree of immunocompromise for the patient is determined by the treating provider, and preventive actions are tailored to each individual and situation.
What is the appropriate length of time between recovery from COVID-19 and surgery with respect to minimizing postoperative complications?
The preoperative evaluation of a surgical patient who is recovering from COVID-19 involves optimization of the patient’s medical conditions and physiologic status. Since COVID-19 can impact virtually all major organ systems, the timing of surgery after a COVID-19 diagnosis is important when considering the risk of postoperative complications.
There are limited data now that address timing of surgery after COVID-19 infection. One study found a significantly higher risk of pulmonary complications within the first four weeks after diagnosis (1). An upper respiratory infection within the month preceding surgery has previously been found to be an independent risk factor for postoperative pulmonary complications (2). Patients with diabetes are more likely to have severe COVID-19 disease and are more likely to be hospitalized (3,4). Studies conducted during the 2009 influenza A H1N1 pandemic found that pulmonary function continues to recover up to three months after ARDS (5).
Given this current knowledge base, wait times before surgery can be reasonably extrapolated and are a suggested starting point in the preoperative evaluation of the COVID-19-recovered patient.
The timing of elective surgery after recovery from COVID-19 utilizes both symptom- and severity-based categories. Suggested wait times from the date of COVID-19 diagnosis to surgery are as follows:
- Four weeks for an asymptomatic patient or recovery from only mild, non-respiratory symptoms.
- Six weeks for a symptomatic patient (e.g., cough, dyspnea) who did not require hospitalization.
- Eight to 10 weeks for a symptomatic patient who is diabetic, immunocompromised, or hospitalized.
- Twelve weeks for a patient who was admitted to an intensive care unit due to COVID-19 infection.
These timelines should not be considered definitive; each patient’s preoperative risk assessment should be individualized, factoring in surgical intensity, patient co-morbidities, and the benefit/risk ratio of further delaying surgery.
Residual symptoms such as fatigue, shortness of breath, and chest pain are common in patients who have had COVID-19 (6,7). These symptoms can be present more than 60 days after diagnosis (7). In addition, COVID-19 may have long term deleterious effects on myocardial anatomy and function (8). A more thorough preoperative evaluation, scheduled further in advance of surgery with special attention given to the cardiopulmonary systems, should be considered in patients who have recovered from COVID-19 and especially those with residual symptoms.
Is repeat SARS-CoV-2 testing needed?
At present, the CDC does not recommend re-testing for COVID-19 within 90 days of symptom onset (9). Repeat PCR testing in asymptomatic patients is strongly discouraged since persistent or recurrent positive PCR tests are common after recovery. However, if a patient presents within 90 days and has recurrence of symptoms, re-testing and consultation with an infectious disease expert can be considered.
Once the 90-day recovery period has ended, the patient should undergo one pre-operative nasopharyngeal PCR test ideally ≤ three days prior to the procedure.
References
- COVIDSurg Collaborative. Delaying surgery for patients with a previous SARS‐CoV‐2 infection. BJS 2020; 107: e601–e602. https://doi.org/10.1002/bjs.12050
- Canet J, Gallart L, Gomar C, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology 2010;113:1338. https://doi.org/10.1097/ALN.0b013e3181fc6e0a
- Guan WJ, Liang WH, Zhao Y, et al. Comorbidity and its impact on 1590 patients with Covid-19 in China: a nationwide analysis. Eur Respir J 2020. DOI: 10.1183/13993003.00547-2020
- Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ 2020;369:m1966 doi: https://doi.org/10.1136/bmj.m1966.
- Hsieh M-J, Lee W-C, Cho H-Y, et al. Recovery of pulmonary functions, exercise capacity, and quality of life after pulmonary rehabilitation in survivors of ARDS due to severe influenza A (H1N1) pneumonitis. Influenza and other respiratory viruses. Apr 2018. https://doi.org/10.1111/irv.12566
- Tenforde MW, Kim SS, Lindsell CJ., et al. Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network – United States, March-June 2020. MMWR 2020 Jul 31;69(30):993-998. https://dx.doi.org/10.15585%2Fmmwr.mm6930e1
- Carfi A, Bernabei R, Landi F., et al. Persistent Symptoms in Patients After Acute COVID-19. JAMA July 9, 2020. doi:10.1001/jama.2020.12603
- Puntmann VO, Carerj ML, Wieters I, et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020;5(11):1265-1273. doi:10.1001/jamacardio.2020.3557
- https://www.cdc.gov/coronavirus/2019-ncov/hcp/duration-isolation.html
Accessed Oct 28, 2020
Table 1: Definitions for Severity Levels of COVID-Related Illness
The studies used to inform the guidance in this joint statement do not clearly define “severe” or “critical” illness. The definitions in the National Institutes of Health (NIH) COVID-19 Treatment Guidelines (cited under references below) are suggested to categorize disease. The highest level of illness severity experienced by the patient at any point in their clinical course should be used.
* Mild Illness: Signs and symptoms of COVID-19 (e.g., fever, cough, sore throat, malaise, headache, muscle pain) without shortness of breath, dyspnea, or abnormal chest imaging.
* Moderate Illness: Evidence of lower respiratory disease by clinical assessment or imaging and oxygen saturation (SpO2) ≥94 percent on room air at sea level.
** Severe Illness: Respiratory rate >30 breaths per minute, SpO2 <94 percent on room air at sea level (or, for patients with chronic hypoxemia, a decrease from baseline of >3 percent), a ratio of arterial partial pressure of oxygen to fractional inspired oxygen (PaO2/FiO2) <300 mmHg, or lung infiltrates involving >50 percent of the lung fields.
** Critical Illness: The presence of respiratory failure, septic shock, and/or multiple organ dysfunction.
*** The studies used to inform this guidance did not clearly define “severely immunocompromised.” For the purposes of this guidance, “severely immunocompromised” refers to patients:
-
- Currently undergoing chemotherapy for cancer.
- Within 1 year of receiving a hematopoietic stem cell or solid organ transplant.
- Having untreated HIV with a CD4 T lymphocyte count <200.
- Having a combined primary immunodeficiency disorder.
- Treated with prednisone >20mg/day for more than 14 days.
Reference sources from CDC and NIH websites as of 22 Sept 2020:
Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19)
https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html
Overview of testing
https://www.cdc.gov/coronavirus/2019-ncov/hcp/testing-overview.html
Discontinuation of Transmission-Based Precautions and Disposition of Patients with COVID-19 in Healthcare Settings (Interim Guidance)
https://www.cdc.gov/coronavirus/2019-ncov/hcp/disposition-hospitalized-patients.html
Duration of Isolation and Precautions for Adults with COVID-19
https://www.cdc.gov/coronavirus/2019-ncov/hcp/duration-isolation.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fcommunity%2Fstrategy-discontinue-isolation.html
National Institutes of Health (NIH) COVID-19 Treatment Guidelines
https://www.covid19treatmentguidelines.nih.gov/whats-new/
What does efficiency in healthcare delivery mean? Examples of two market failures
October 08, 2021 3:41 pm
Introduction:
Economic efficiency measures system performance (Enrique & Marta, 2020); the Healthcare delivery system (HCDS) is no different. In non-biologic systems, the efficiency can be measured and optimized since all variables are predictable. However, efficiency becomes a complex and possibly unachievable task in a biological environment such as HCDS. The summary report will define the efficiency and examine the limitation of achieving efficiency in the healthcare delivery system.
Definitions:
Efficiency measures the adeptness of a system allowing identification of the inadequacies and opportunities for improvement. Economic efficiency minimizes cost and maximizes production for profit (Petrou, 2014).
Healthcare is a commodity (Mills & Gilson, 2009). Increased need and limited resources, environment, illnesses are forces on an equilibrium of efficiency that requires flexibility. These are why economically competitive markets fail to achieve healthcare efficiency (Johansen & van den Bosch, 2017).
The concept of efficiency in health care has been described as Technical, Productive, and Allocative (Palmer & Torgerson, 1999). Extensive work has looked at special measures and populations for optimizing efficiency (Cylus & Papanicolas, 2016).
Efficient systems require predictable input, components, processes, and output, unlike efficiency in HCDS. The differences include:
- Biologic environments introduce variability in the system. Therefore, the HCDS efficiency will need to be flexible to diversity. Unfortunately, flexibility and efficiency counteract each other at industrial levels (Adler et al., 1999; AHRENS & CHAPMAN, 2004), and thus inefficiency is to be expected.
- Efficiency can be measured at two points:
- Efficiency of delivery
- Efficiency of outcome
Efficiency in HCDS means providing the most cost-efficient healthcare to those in need. As equity is a pillar of the HCDS, efficiency and equity are opposing forces (Guinness et al., 2011). Therefore, it is critical to have the broader determinants of health into consideration on HCDS. This broad spectrum of variables, individual level, and upstream factors (Dahlgren G & Whitehead M, 1991) will affect efficiency models applicable in one setting for a given population and inefficient in another (Hussey et al., 2009).
Healthcare Market:
The principle of maximizing profits applies to the four market types[1][2]. However, healthcare markets achieve Social Efficiency[3] and not economic efficiency (Folland & Goodman, 2013). This is due to Asymmetry of the information, Adverse selection, Moral hazard, Independent supply and demand stresses, and Externalities (Mwachofi & Al-Assaf, 2011).
Examples of Market Failure
At the onset of the pandemic, most governments, WHO assumed the costs of COVID-19 vaccination as they became available. Social media has disseminated incorrect information on vaccines (Lin et al., 2020; Wajahat Hussain, 2020). The Asymmetry of the information (AOI) has resulted in a sizable portion of the eligible population not being vaccinated (Coe et al., 2021; Malik et al., 2020). HCDS’s failure is a public relations problem and a breakdown in the trust of institutions (Soares et al., 2021).
Adverse selection (AS) compounds the AOI. There have been pockets of efficiency in vaccination with no equity for the world population (Mathieu et al., 2021).
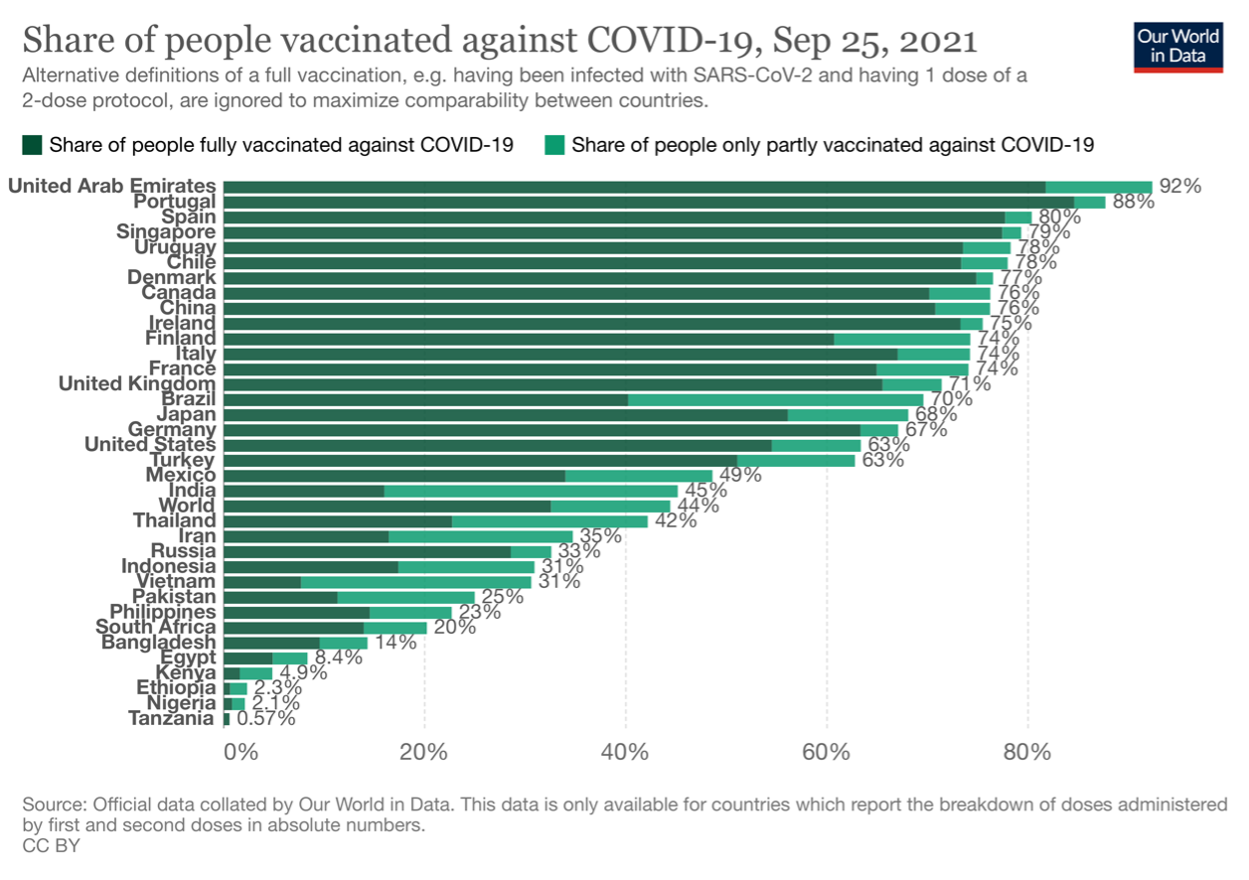 This is due to the AOI and the structural inequities in HCDS (Hyder et al., 2021). Few countries are offering vaccine boosters, where most of the world’s population has not received any.
This is due to the AOI and the structural inequities in HCDS (Hyder et al., 2021). Few countries are offering vaccine boosters, where most of the world’s population has not received any.
References:
Adler, P. S., Goldoftas, B., & Levine, D. I. (1999). Flexibility Versus Efficiency? A Case Study of Model Changeovers in the Toyota Production System. Organization Science, 10(1), 43–68. https://doi.org/10.1287/orsc.10.1.43
Adler, P. S., Goldoftas, B., & Levine, D. I. (1999). Flexibility Versus Efficiency? A Case Study of Model Changeovers in the Toyota Production System. Organization Science, 10(1), 43–68. https://doi.org/10.1287/orsc.10.1.43
AHRENS, T., & CHAPMAN, C. S. (2004). Accounting for Flexibility and Efficiency: A Field Study of Management Control Systems in a Restaurant Chain*. Contemporary Accounting Research, 21(2), 271–301. https://doi.org/https://doi.org/10.1506/VJR6-RP75-7GUX-XH0X
Coe, A. B., Elliott, M. H., Gatewood, S. B. S., Goode, J. V. R., & Moczygemba, L. R. (2021). Perceptions and predictors of intention to receive the COVID-19 vaccine. Research in Social and Administrative Pharmacy. https://doi.org/10.1016/j.sapharm.2021.04.023
Cylus, J., & Papanicolas, I. (2016). Health System Efficiency 46 How to make measurement matter for policy and management. London.
Dahlgren G, & Whitehead M. (1991). Dahlgren and Whitehead (1991) – Policies and strategies to promote social equity in health. Stockholm: Institute for future studies. Dahlgren G, Whitehead M. Retrieved from https://core.ac.uk/display/6472456
Enrique, B., & Marta, B. (2020). Efficacy, Effectiveness and Efficiency in the Health Care: The Need for an Agreement to Clarify its Meaning. International Archives of Public Health and Community Medicine, 4(1). https://doi.org/10.23937/2643-4512/1710035
Folland, S., & Goodman, A. (2013). The Economics of Health and Health Care. Oakland: Pearson.
Guinness, L., Wiseman, V., & Wonderling, D. (2011). Introduction to health economics. (2nd ed. /). Maidenhead: McGraw-Hill/Open University Press.
Hussey, P. S., de Vries, H., Romley, J., Wang, M. C., Chen, S. S., Shekelle, P. G., & McGlynn, E. A. (2009). A systematic review of health care efficiency measures. Health Services Research, 44(3), 784–805. https://doi.org/10.1111/j.1475-6773.2008.00942.x
Hyder, A. A., Hyder, M. A., Nasir, K., & Ndebele, P. (2021). Inequitable COVID-19 vaccine distribution and its effects. Bulletin of the World Health Organization, 99(6), 406-406A. https://doi.org/10.2471/BLT.21.285616
Johansen, F., & van den Bosch, S. (2017). The scaling-up of Neighbourhood Care: From experiment towards a transformative movement in healthcare. Futures, 89, 60–73. https://doi.org/https://doi.org/10.1016/j.futures.2017.04.004
Lin, C. Y., Broström, A., Griffiths, M. D., & Pakpour, A. H. (2020). Investigating mediated effects of fear of COVID-19 and COVID-19 misunderstanding in the association between problematic social media use, psychological distress, and insomnia. Internet Interventions, 21. https://doi.org/10.1016/j.invent.2020.100345
Malik, A. A., McFadden, S. A. M., Elharake, J., & Omer, S. B. (2020). Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine, 26. https://doi.org/10.1016/j.eclinm.2020.100495
Mathieu, E., Ritchie, H., Ortiz-Ospina, E., Roser, M., Hasell, J., Appel, C., … Rodés-Guirao, L. (2021). A global database of COVID-19 vaccinations. Nature Human Behaviour, 5(7), 947–953. https://doi.org/10.1038/s41562-021-01122-8
Mills, A., & Gilson, L. (2009). Health Economics for Developing Countries: A Survival Kit. Esocialsciences.Com, Working Papers.
Mwachofi, A., & Al-Assaf, A. F. (2011). Health care market deviations from the ideal market. Sultan Qaboos University Medical Journal, 11(3), 328–337. Retrieved from https://pubmed.ncbi.nlm.nih.gov/22087373
Palmer, S., & Torgerson, D. J. (1999). Economic notes: definitions of efficiency. BMJ (Clinical Research Ed.), 318(7191), 1136. https://doi.org/10.1136/bmj.318.7191.1136
Petrou, A. (2014). Economic Efficiency. In A. C. Michalos (Ed.), Encyclopedia of Quality of Life and Well-Being Research (pp. 1793–1794). Dordrecht: Springer Netherlands. https://doi.org/10.1007/978-94-007-0753-5_818
Soares, P., Rocha, J. V., Moniz, M., Gama, A., Laires, P. A., Pedro, A. R., … Nunes, C. (2021). Factors associated with COVID-19 vaccine hesitancy. Vaccines, 9(3). https://doi.org/10.3390/vaccines9030300
Wajahat Hussain. (2020). Role of Social Media in COVID-19 Pandemic. The International Journal of Frontier Sciences, 4(2), 59–60. https://doi.org/10.37978/tijfs.v4i2.144
[1] Perfect competition, Monopoly, Oligopoly, Monopolistic competition
[2] Control of Total revenue (TR) and Cost (TC) to maximize profit
[3] An equilibrium point (Pareto Optimality) where Social Marginal Benefit (SMB) and the Cost (SMC) are equal
Zoom Group Meeting November 24, 2020
November 24, 2020 4:40 pm
 Link to CDC website.
What is PCR – Polymerase Chain Reaction:
Link to CDC website.
What is PCR – Polymerase Chain Reaction: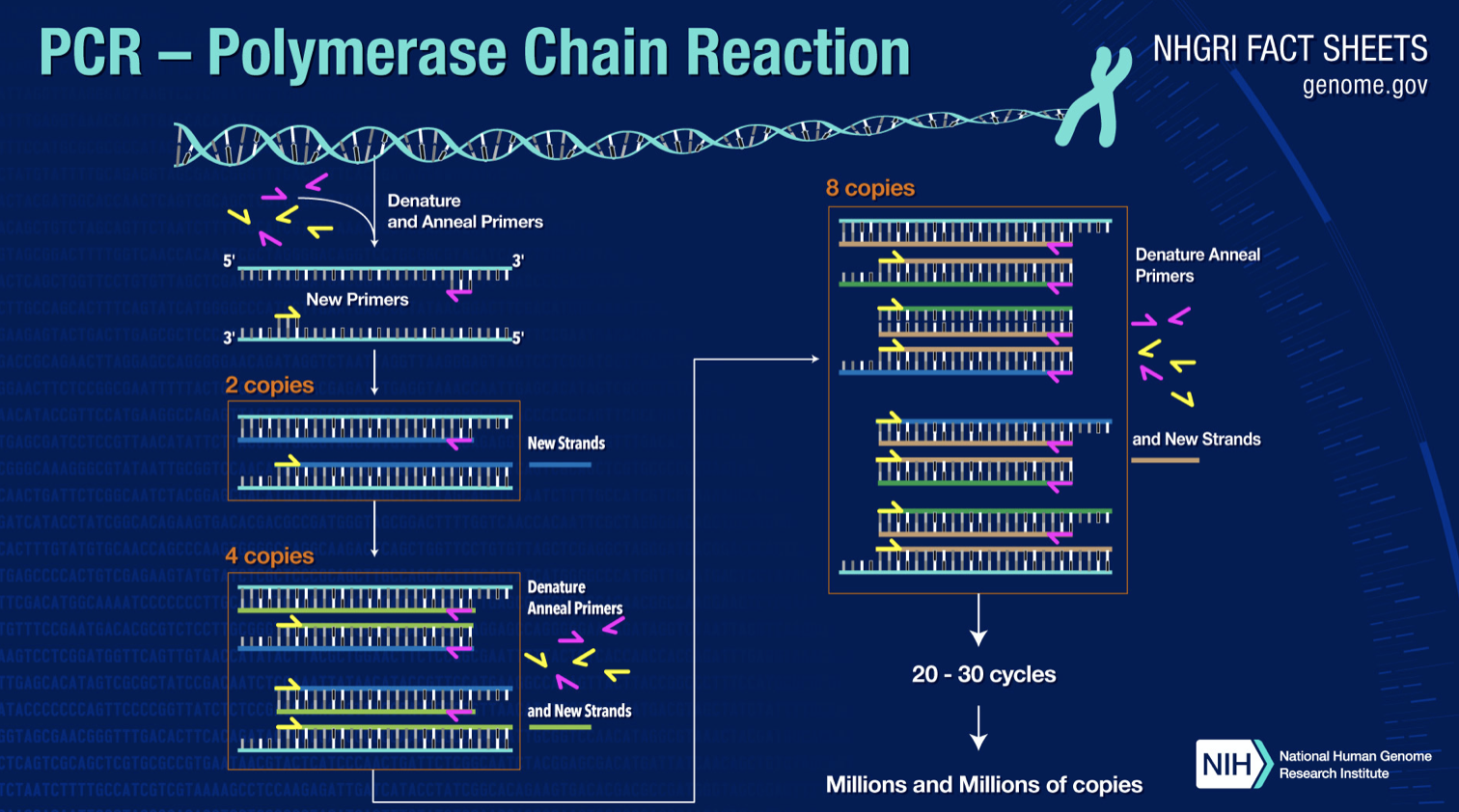 Types of Vaccines….
“The final two vaccine candidates (from Moderna and BioNTech/Fosun Pharma/Pfizer) are mRNA vaccines. What are those?
First it helps to remember that DNA is the gene and RNA gives instructions for certain proteins. So an mRNA vaccine is the instructions for the SARS-CoV2 protein. Once inside the cell, the protein is made and that triggers the immune response. Just like the vector vaccines which use viruses to deliver the protein instructions, here you are delivering the instructions alone. It’s another way of getting the protein made inside of you.
Is there any risk of getting COVID-19 or COVID-19-like side effects from these vaccines?
When people talk about side effects of a vaccine, people often believe you’re getting a weaker version of the virus and a minor version of the disease. That is not what these things do. Most vaccine side effects — which include anything from a sore arm, to feeling warm to muscle aches — are a sign of the immune response. It’s not that you get a mild form of the disease. That’s important to be clear about. People keep a very close eye because you want to make sure these vaccines are safe.”
https://labblog.uofmhealth.org/rounds/top-5-covid-19-vaccine-candidates-explained
Types of Vaccines….
“The final two vaccine candidates (from Moderna and BioNTech/Fosun Pharma/Pfizer) are mRNA vaccines. What are those?
First it helps to remember that DNA is the gene and RNA gives instructions for certain proteins. So an mRNA vaccine is the instructions for the SARS-CoV2 protein. Once inside the cell, the protein is made and that triggers the immune response. Just like the vector vaccines which use viruses to deliver the protein instructions, here you are delivering the instructions alone. It’s another way of getting the protein made inside of you.
Is there any risk of getting COVID-19 or COVID-19-like side effects from these vaccines?
When people talk about side effects of a vaccine, people often believe you’re getting a weaker version of the virus and a minor version of the disease. That is not what these things do. Most vaccine side effects — which include anything from a sore arm, to feeling warm to muscle aches — are a sign of the immune response. It’s not that you get a mild form of the disease. That’s important to be clear about. People keep a very close eye because you want to make sure these vaccines are safe.”
https://labblog.uofmhealth.org/rounds/top-5-covid-19-vaccine-candidates-explained