
Category: surgical nutrition
Length of Bowel : Hess or No Hess
March 22, 2020 5:58 pm
“…What is the length of my common channel” is probably one of the frequently asked questions about the duodenal switch operation in the office. This usually comes up at the initial consult when patients repost credible sources such as Dr. Google and Dr. Facebook for patient with different bowel length have done well or not so after duodenal switch operation. Dr. Hess described the Duodenal Switch by using total bowel length measurements and creating the common channel as a percentage of the total small bowel length. However, it seems that this is being done less and less.
This leads to my explanation that is on the website
Hess calculator : Bowel Length Calculator
How the actual measurements matters: Bowel length video link
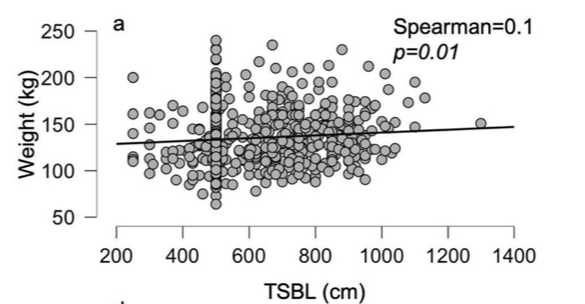
In 2019, Bekheit et.al published a very interesting study comparing total small bowel length (TSBL) to a number of variables such as height, weight, sex and BMI. They identified a few loose correlations. Male patient have longer TBSL than females. There was correlation between TSBL and height stronger in males than females but not statistically significant.
In Conclusion they reported ” Despite statistical significance of the correlation between the TSBL and the height and weight of the included participants, the correlation seems to have no clinical meaning since the effect size is negligible. ”
As I have previously discussed this Making the common and alimentary length standard for every duodenal switch patient will make some loose too much and other not enough weight.
Figure 1 shows TSBL on the horizontal axis, and height, weight, BMI and Age on the vertical axis. For the most part what they all show is that one can not predict how long a patients bowel is by any of the measures that we take in the office as a part of the routine exam.
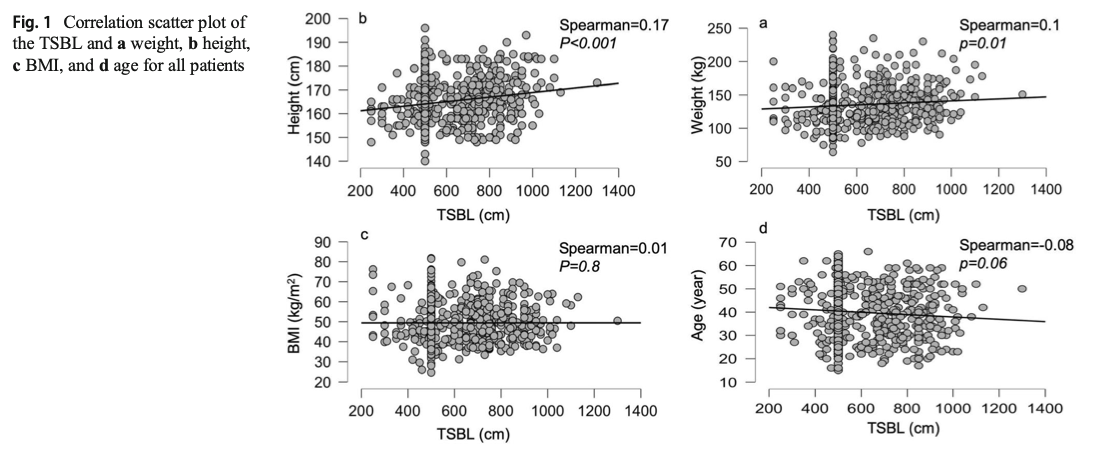
This raises, the concerns that I had raised previously. How could two similar patients who have the same weight, age, sex and BMI have the same surgery and expect the same result if one of them has TSBL of 400 cm and the other one 800cm?
 If both of the patients get the same “cookie cutter” duodenal switch with the same lengths, then the patient with TSBL of 400 will have much longer common channel if the surgeon does not customize the length of the bowel. This is an example of many patients whom we have revised over the years where they had a duodenal switch done with the “standard” 125cm common channel and when we measured the total length the patient had 500 cm TSBL.
If both of the patients get the same “cookie cutter” duodenal switch with the same lengths, then the patient with TSBL of 400 will have much longer common channel if the surgeon does not customize the length of the bowel. This is an example of many patients whom we have revised over the years where they had a duodenal switch done with the “standard” 125cm common channel and when we measured the total length the patient had 500 cm TSBL.
Parathyroid Scan
July 09, 2018 11:48 am
A Parathyroid scan or Sestamibi scan may be needed if the typical weight loss surgical reasons for elevated PTH levels have been addressed. Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with overactive parathyroid and is absorbed by the overactive parathyroid gland. If the parathyroid is normal it will not absorb the agent. The scan below shows the uptake of the agent.
Calcium, Vitamin D and Parathyroid hormone are routinely measured on yearly follow up for most post weight loss surgical (WLS) patients. Elevated parathyroid hormone (PTH) may be caused by Vitamin D deficiency or calcium deficiency (most common in post WLS) or by over active parathyroid gland(s). In the latter case, if one of the four glands is overactive then this is knows as a parathyroid Adenoma. If all 4 are over active and are secreting too much PTH, this is known as hyperplasia. Ultrasound of the neck, may identify an enraged parathyroid gland (adenoma) which is located behind the thyroid gland. Given the large area where the parathyroid gland may be located, additional tests are needed to not only identify the location of the gland(s) but also to distinguish between single gland (adenoma) or multiple glands (hyperplasia) cause for the elevated PTH. It is important to investigate all avenues and testing in parathyroid hormone elevation and in some cases, not to rely on one test for your diagnosis. It is also imperative that weight loss surgical patients take their supplements routinely and consistently and have their laboratory studies followed at least yearly.

Zinc InformationExclusive Member Content
April 17, 2015 7:22 am
Stages of Liver Failure
January 08, 2013 9:38 pm
The liver is probably one of the most forgiving organs when it comes to recovering from an injury. It can take a significant amount of “non structural” injuries and still be able to carry out its function. It is the only solid organ capable of regenerating its volume after a major resection. When a part of the liver is removed, it is within a matter of months that the size of the remaining liver increases to replace the removed portion.
A liver injury can be caused by a number of elements. In regards to weight loss surgery, these elements include alcohol consumption, high doses of Tylenol, excessive weight loss, and the most significant condition called steatohepatitis, also known as “fatty infiltration”. Steatohepatitis causes structural changes in the liver. Over time, the structural changes cause the liver to progress to an end-stage liver disease that requires a transplant. Structural changes to the liver injury are irreversible.
The healthy liver is normally soft and beefy-red with a very smooth and shiny outer layer.
How does steatohepatitis harm the liver? As the fat concentration of the liver increases, the liver loses its sharp edge and becomes distended with small pockets of fat that are visible as yellow satellite lesions.





The healthy liver is normally soft and beefy-red with a very smooth and shiny outer layer.
How does steatohepatitis harm the liver? As the fat concentration of the liver increases, the liver loses its sharp edge and becomes distended with small pockets of fat that are visible as yellow satellite lesions.
This is gross evidence of steatohepatitis, which is commonly known as fatty infiltration of the liver. The most common cause of this is obesity, in addition to medications such as insulin that are used to treat diabetes. If the underlying cause of steatohepatitis is not addressed, then the liver damage will progressively continue to worsen and eventually be resolved in the structural changes to the liver.
If the physiologic injury to the liver continues unabated, it will develop irreversible cirrhosis. An increasingly continuous insult to the liver will result in sudden liver failure, which will require a liver transplant.
Feeding Jejunostomy TubeExclusive Member Content
February 06, 2012 3:38 am
Sleeve Gastrectomy post operative diet
January 03, 2012 11:15 pm
A relatively common question asked post operatively regards the pace at which the post operative diet should be advanced. In our practice, patients are given a simple list describing 3 broad categories. They are outlined in the work book.
Each patient should advance his or her diet over a 1-4 weeks in the post operative timeframe. The most important point to remember is that each one of us responds differently to the food at a certain point following surgery. The safest method to advance the diet would be to pay attention to what your body is telling you. If a patient is tolerating Bariatric 1 and Bariatric 2 diet, then they should be able to advance to a soft diet in one or two weeks. Alternatively, if the patient is having difficulty getting their required water on a daily basis, then advancing to a soft diet may be an incorrect move at that point.The basic order of food is water, protein, and everything else.
Pizza versus SaladExclusive Member Content
January 30, 2011 9:01 pm