
Category: revision of AGB
COVID Vaccines
March 05, 2021 3:50 pm
There are no known contraindications from a weight-loss surgical perspective to prevent a post-surgical patient from getting the COVID vaccines.
A patient who has had a Duodenal Switch, Lap Sleeve Gastrectomy, RNY Gastric Bypass, or revisions to Weight Loss Surgery should have the COVID vaccine. The vaccination should be avoided for a few weeks after surgery. For other possible contraindications, please consult your PCP.
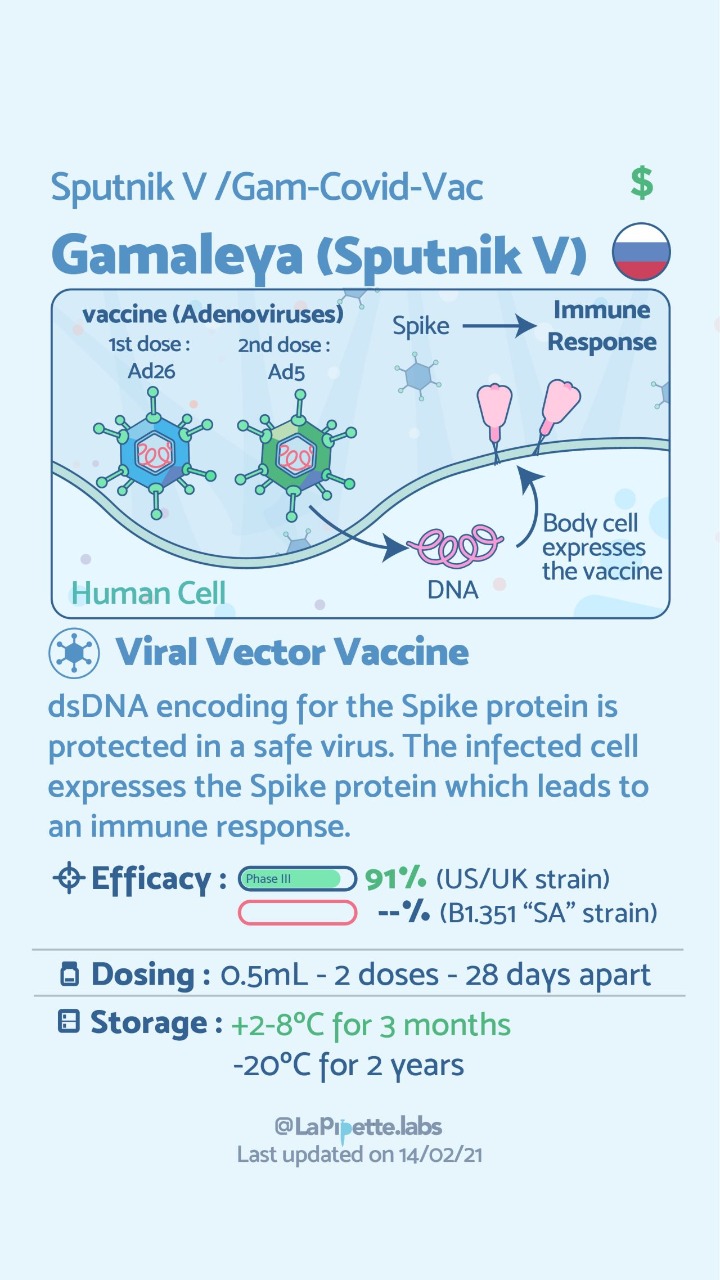
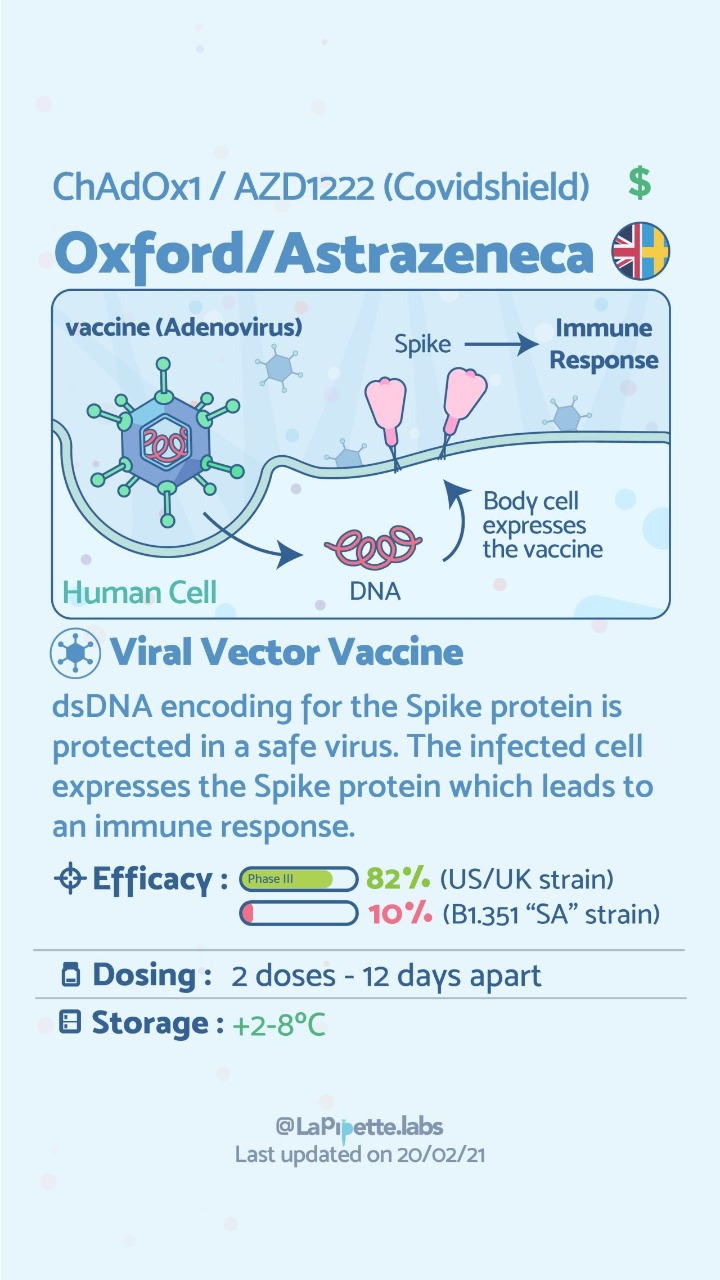
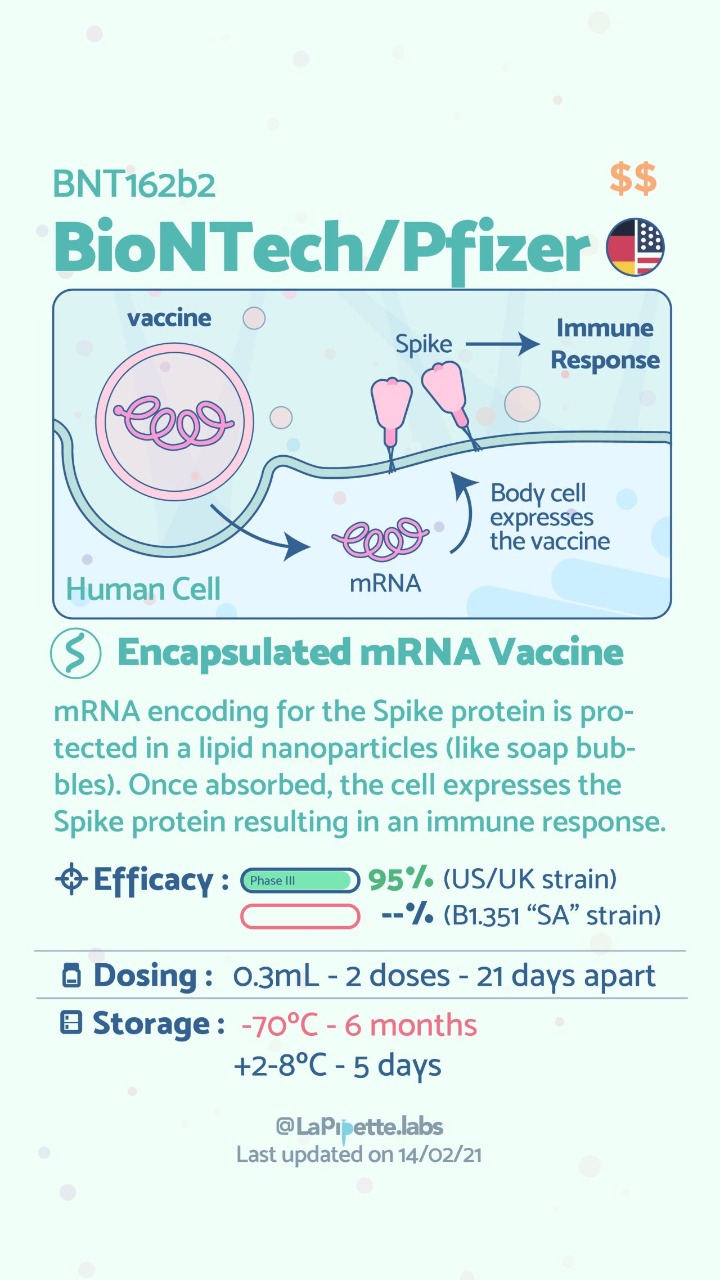
Here is a summary of the vaccines and the details of each one approved as of the publication date.



Zoom Group Meeting
September 21, 2020 7:10 am
We are excited to announce we will be having a Zoom group meeting Tuesday, September 22, 2020 at 7:00 PM PST. We hope to see you online!
Registration is required. Please follow the link to the meeting registration.
Cholecystectomy-Gallbladder Removal
September 10, 2018 9:44 am
There are differing opinions, based on a broad set of scientific publication, wether or not gallbladder should be removed at the time of weight loss surgery. Obviously, Cholecystectomy is a stand alone general surgical procedure that is often performed due to gallstones and/or gallbladder disease with a variety of symptoms. However, the focus of this blog will deal with Bariatric Surgery and Cholecystectomy.
Rapid weight loss can increase a patients chance of forming gallstones. This rapid weight loss can be as little as 3-5 pounds per week. Weight loss surgery can increase your risk for gallstone formation. Several of the common thought processes the mechanism of this is, obesity may be linked to higher cholesterol in the bile, larger gallbladders, high fat diet and larger abdominal girth.

When a patient is having the Duodenal Switch (DS) Bariatric operation, or having a revision of a failed gastric bypass to the DS, I always remove the gallbladder. This is because there isn’t an anatomical route to utilize endoscopic procedure for an ERCP should the need rise.
In the case of a patient undergoing Vertical Sleeve Gastrectomy, if there are any indications or complaints of abdominal pain then an ultrasound is done. If there are findings of gallstones or other disease of the gallbladder, then a cholecystectomy is performed at the same time as the Sleeve Gastrectomy.


In my opinion, every patient having the Gastric Bypass (RNY) should also have the gallbladder removed because of the anatomical limitations after surgery that prevents the use of ERCP if needed. Some clinicians will place the patient on a long term medications to reduce the chance of gladstone formation after surgery, which themselves have side effects limiting the compliance in most patients.
Further information on Common Bile Duct Dilatation and ERCP
Parathyroid Scan
July 09, 2018 11:48 am
A Parathyroid scan or Sestamibi scan may be needed if the typical weight loss surgical reasons for elevated PTH levels have been addressed. Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with overactive parathyroid and is absorbed by the overactive parathyroid gland. If the parathyroid is normal it will not absorb the agent. The scan below shows the uptake of the agent.
Calcium, Vitamin D and Parathyroid hormone are routinely measured on yearly follow up for most post weight loss surgical (WLS) patients. Elevated parathyroid hormone (PTH) may be caused by Vitamin D deficiency or calcium deficiency (most common in post WLS) or by over active parathyroid gland(s). In the latter case, if one of the four glands is overactive then this is knows as a parathyroid Adenoma. If all 4 are over active and are secreting too much PTH, this is known as hyperplasia. Ultrasound of the neck, may identify an enraged parathyroid gland (adenoma) which is located behind the thyroid gland. Given the large area where the parathyroid gland may be located, additional tests are needed to not only identify the location of the gland(s) but also to distinguish between single gland (adenoma) or multiple glands (hyperplasia) cause for the elevated PTH. It is important to investigate all avenues and testing in parathyroid hormone elevation and in some cases, not to rely on one test for your diagnosis. It is also imperative that weight loss surgical patients take their supplements routinely and consistently and have their laboratory studies followed at least yearly.

Revision from failed AGB to Duodenal Switch
January 10, 2018 2:10 pm
A few times a month during consultation for weight loss surgery , I’m ask as to why I do not offer the adjustable gastric banding as an alternative to the patients. As I have said over the years when a patient considers an weight loss surgery the totality of the risk should be considered. This includes the operative, immediate postoperative course, the maintenance and the follow-ups needed. The potential complications of the procedure in addition to the long-term success off each operation should also be taken into account.
Unfortunately, some patients are led to believe that any perceived benefit in the short operative time and the ease of the adjustable gastric banding also translates to a better outcome. This is in fact the opposite of what the published data have shown, a recent study published in April 2017 by Vinzes et.al, shows that 71% of patient lost their band by 10 years out.




What is also interesting that more patients underwent revision from failed AGB to the duodenal switch than the sleeve gastrectomy (Fig 1.). This is what I also recommend.
More importantly, The patients who underwent a revision from failed AGB to the duodenal switch operation had the best long term results of all patients (Fig 2.) note the “rBPD” line that is the highest of %EBMIL.
Complication’s were broad and frequent (Table 3.)
Further information on revision from failed AGB to Duodenal Switch or other failed weight loss surgeries can be found here.
Long Term Complications of Adjustable Gastric Banding
October 17, 2017 6:35 am
It is interesting to encounter patients who are still being recommended for Lap Band placement to treat morbid obesity. There is a vast body of scientific evidence supporting that Lap Band not only does not result in a sustained weight loss for majority of the patients, but that it results in significant long term complications for some.
One of the complications is a significant stricture (narrowing) where the band is located even when it is completely empty. This is cause by:
1- either scarring of the tissue around that band causing a “belt” effect around the stomach, or


There are numerous other complications that are associated with Adjustable Gastric Bands that encompass a wide range of areas that are not discussed in this blog. This recent article (yes another one) outlines the dismal long term outcome of the Adjustable Gastric banding- Buyer Beware.
https://www.dsfacts.com/pdf/agb-long-term-results-1506834076.pdf
New Pasadena Office Map and Parking
August 12, 2017 8:35 am
We’ve created a helpful map and parking diagram for our new Pasadena, CA office location. It also has a general layout of the Huntington Memorial Hospital Campus and Pre-operative intake and testing area. We hope that you find it helpful on your next visit to see Dr. Ara Keshishian, General and Bariatric Surgeon.

Dr. Ara Keshishian has performed more than 2,000 Duodenal Switch procedures, thousands of Sleeve Gastrectomies and more than 500 revisions from other Weight Loss Surgeries such as RNY Gastric Bypass, Adjustable Gastric Band, and Sleeve Gastrectomy to Duodenal Switch as well as General Surgical cases over the last 18 years of private practice.
Gastric Band Complications
June 21, 2017 10:22 am
For years, we have seen patients who have had Adjustable gastric bands placed and continue to suffer from the complications associated with it. Gastric Band complications include erosion, persistent nausea, vomiting abdominal pain, inadequate weight loss and weight regain, etc. . Unfortunately, when seeking help, they are often told that this never happens to others and that complications are a rare occurrence. Let’s remember that the Adjustable Gastric Band was promoted and sold as a procedure with almost no down side, low risk and easily revisable!
There is an unfounded expectation that the band can be deflated and all the Gastric Band complications will resolve. This could not be any further from the truth. The reality is that there are patients whose symptoms may somewhat improve but will continue to have the abdominal pain, the nausea and or vomiting-albreit, not to the same intensity. There are several Gastric Band complications that are considered emergency situations that require immediate attention by a physician.
Our position has always been, and continues to be, that all Adjustable Gastric Bands should be removed by a surgeon who is experienced with the Gastric Band complications and revisions.
")
")
")
Success Story: Hasmik
January 13, 2016 2:47 pm
Failed Band: My earliest memory of feeling ashamed of being “too heavy” is from kindergarten. For over 30+ years I have struggled with gaining weight, trying to lose weight, or going mad maintaining my weight. There is no shortcut that does not come back to bite you in the butt. There is no diet that effectively changes you permanently. For me exercise is a mindful struggle I sometimes successfully commit to over small periods of time.
I was desperate and ready for a real change. I wanted a genuine difference in the way I consumed and related to food and decided the lap band was the way to go. It was marketed as a “non intrusive, non permanent, easily reversible weight loss tool” and that is EXACTLY what I thought I needed and wanted. I was so very wrong, after my surgery I was considered a “success”. In fact up until the removal of my second slipped failed band, esophagus damage, and poor nutrition; I was considered a success. I look back and think how troubling this was/is. How very damaging to the person struggling and dealing with weight issues. Truly, it messed with my mind and my ability to speak up, admit to myself and out loud the band was NOT working for me. In fact, if I’m completely truthful, it was dangerous and turned me into a residue of the person I once was. I was not able to eat comfortably or eat out any place I happen to be. With the Band, I would need to consider how long I was going to be away from home because I could only eat small bites in small quantities to ensure I did not get stuck or worse vomit what I put inside my mouth. Yes, I had lost almost 100 lbs, but I had given my quality of life as payment. My guilt ensured I would never speak up or complain since I felt “fortunate” and grateful to have had this second chance at life. In my mind, speaking up meant possibly losing the tool (lap band) that allowed me to change my life and reality. Because for the first time in memory, I was the same weight at the start, middle, and end of the year. I did not have to buy different sizes of clothing or underclothing. I could predict what I might wear since my size was stable and my clothes fit. The reality is and was far from this corrupted self truth. I was unhealthy with the restrictive nature of how the lap band worked. In fact my band slipped twice after a severe stomach virus. I later learned of many other symptoms I was making excuses for and quite frankly straight out ignored.
I met Dr. Keshishian (Dr. K) at my lowest weight and at the lowest point in my health. I finally realized, the lap band needed to come out after it had slipped again. It was clear I needed a doctor who would be straight with me and cared for my health and not his/her “success” rates and have the expertise to deal with my failed band. I researched and called several bariatric surgeons then attempted to make appointments with each to discuss the urgent band removal surgery I needed (not as simple as you would think). I was also hopeful I might have the option to undergo the bariatric sleeve surgery because I knew I would not be able to keep my weight under control on my own. I was unwilling to undergo the emotional and mental torment of gaining and losing weight for the rest of my days. I succeeded in making three appointments and truthfully after meeting and speaking to Dr. K and his office staff I canceled them immediately. Let me start with the staff as that REALLY is important; they help you feel comfortable with the doctor, the procedure, and overall experience. They represent and reflect how the doctor you’re about to see will treat his patients. The expected standard within Dr. Keshishian’s office immediately made me feel like I called the right place. I was taken by the knowledgable, kind tone and efficient manner in which they requested the necessary information to effectively help me get from the starting point to the end goal. When I got to my appointment, Dr. Keshishian BLEW MY MIND. He not only presented himself as an approachable person I immediately felt at ease with but also reveal my concerns and questions. He treated me like a person. This may sound strange but this doctor made me feel like a human being with real concerns. He listened to me, asked questions rather than talked at me, and explained how and what was happening to my body and mind. He spent 3 hours with me to answer all my questions (even if I repeated them), draw diagrams, show me video to better help me understand what was happening, and then just sat with me while I cried for a moment. I cried because my 30+ years journey of ups and downs, crazy and insanity finally led me to the door of a man who understood and knew how to help without judgment. WHICH DOCTOR DOES THIS! None that I know.
My life post surgery is what I always hoped it would be. I am able to eat vegetables, leafy greens, fruit, grains and basically a well rounded diet. What’s amazing is that I naturally do not crave sweets, heavy creamy dressings, sauces and fill up quickly. There is after all a difference between the restriction of a lap band and the feeling of being full with the sleeve which Dr. K patiently explained. Today I am able to go any where, at any time, enjoy the moment and the company rather than worry about what I’m not able to consume. My days of scanning to locate the nearest bathroom in case I need to dash to it are over.
As I write this today, I feel like a real person, not some transient hoping to savor my life at glimpses. I am a person that is balanced in my heart with the average person’s anxiety and mindful eating habits. The sleeve is not a magic end to weight gain, it does give you the fighting chance to make choices in life leading up to results you’re willing to work for.
~ Grateful and Mindful, Hasmik (September 2015 Sleeve Op Patient)
2015 ASMBS Summary
November 11, 2015 7:31 am
The 2015 ASMBS meeting was held November 2-6, 2015. It was combined with TOS (The Obesity Society) and had more than 5,600 attendees from all over the world in every aspect of obesity treatment. There were some interesting additions and deletions from this meeting compared to the past.
The one sentence that comes to my mind is “I told you so”.
One important addition was a DS course for Surgeons and Allied Health. This was very exciting, except the content and questions seemed to gravitate to SADI/SIPS/Loop rather than DS. Dr. Cottam was one of the moderators of the course. It seems that they have found the value in preserving the pyloric valve. It was clear that the discussion was driven by the need to come legitimize the single anastomosis procedures at this early stage with almost no data to prove long term outcome. With many of the Vertical Sleeve Gastrectomies having re-gain and the they are looking for a surgery that the “masses” can perform. This was actually the term used by one of the presenters, implying that the duodenal switch needed to be simplified so that all surgeons, those who have pushed all other procedures can not offer Duodenal Switch to their patients with less than desirable outcome. Several surgeons also voiced their concern and dissatisfaction with the issues and complication of the RNY and want an alternative. There was much discussion regarding SADI/SIPS/Loop being investigational and that it shouldn’t be as it is a Sleeve Gastrectomy with a Billroth II. Dr. Roslin and Dr. Cottam discussed their SIPS nomenclature saying they wanted to stay away from something that had Ileostomy, suggesting bowel issues, or the word “SAD”i due to negative connotations. The point to be made is that the SADI and SIPS and the loop are all the same. I have also noticed other surgeons using SADS (Single Anastomosis Duodenal Switch). There is a great deal of industry behind these procedures and many surgeons being trained in courses funded by industry. One surgeon stood up and informed the entire course that they need to be clear with their patients about the surgery they are performing, as he had been in Bariatric chat rooms and there is upset within the community about SADI/SIPS/Loop being toted as “the same or similar to Duodenal Switch”.
There was also presenter who said “We are doing something new about every five years.” No, “we” are not. Some of us have stood by the surgery and techniques with the best long term outcomes and not gone with every “new” thing out there. The process of Duodenal Switch may have changes, open Vs. Lap, drains, location of incisions, post operative care and stay, but the tested procedure with the best outcome has been the duodenal switch operation and not the shortcut versions. Although, those of us that are standing by long term results seems to be in the minority. Why do I stand by Duodenal Switch? Because it works, when done correctly by making the length of the bowel proportional to the patient total bowel length, and height, and not just cookie cutter length for all patients, with the right follow-up, patient education, vitamin and mineral regime and eating habits.
A new addition was the Gastric Balloon, which in the research presented had a 60-70% re-gain rate and a no more than 10-15% weight loss one year only. This data represents more than 70% weight regain when the balloon is taken out. The Gastric Balloons can be left in between 4-6 months depending on the brand or type of balloon. The Gastric Balloon is not new to the Bariatrics and was first introduced in 1985. After 20 years and 3,608 patients the results were and average of 17.6% excess weight loss. It seems that we are re-gurgiating old procedures. There are many new medications that were front and center in this meeting.
The Adjustable Gastric Bands were missing from the exhibit hall this year. It is my hope and feeling from the other attendees that we may be seeing the era of the Adjustable Gastric Band being placed in patients come to an end. Although there are some still holding out that there are some patients that can do well with the Band.
Attending the 2015 ASMBS meeting this year, as it has every year, only reemphasized the importance of avoiding what has become the norm of chasing a simple solution that is fashionable and easy now. We stay convinced that the duodenal switch operation with the common channel and the alimentary length measured as a percentage of the total length is by far the best procedure with the proven track record. The patient should avoid the temptation of settling for an unproven procedure or device, because if history holds true, there will be a need for revision surgeries in the future.