
Category: Nutrition
Cheers! Alcohol Metabolism
December 17, 2024 1:59 pm
Cheers! Let’s take a minute to look at alcohol metabolism. It’s that time of year when it seems we are going from one Holiday or Christmas party to another, and then we get together with the family and have a little more alcohol. The following diagram shows how alcohol metabolism takes place.
Alcohol is a caloric intake, and we all need to keep close tabs on it. Alcohol is very easily metabolized and the calories add up quickly. Every stage of alcohol processing in the liver involves the extraction of calories and free radicals, which are toxins. Excess calories not used in bodily functions can be stored as fat mass. Alcohol can be a roadblock in weight loss. Those drinks add up!


Here is a short video as a reminder while everyone waits to get ready for the next party.
Happy holidays.
A newsletter post from 2004 regarding the effects of alcohol and weight loss surgery.
What does efficiency in healthcare delivery mean? Examples of two market failures
October 08, 2021 3:41 pm
Introduction:
Economic efficiency measures system performance (Enrique & Marta, 2020); the Healthcare delivery system (HCDS) is no different. In non-biologic systems, the efficiency can be measured and optimized since all variables are predictable. However, efficiency becomes a complex and possibly unachievable task in a biological environment such as HCDS. The summary report will define the efficiency and examine the limitation of achieving efficiency in the healthcare delivery system.
Definitions:
Efficiency measures the adeptness of a system allowing identification of the inadequacies and opportunities for improvement. Economic efficiency minimizes cost and maximizes production for profit (Petrou, 2014).
Healthcare is a commodity (Mills & Gilson, 2009). Increased need and limited resources, environment, illnesses are forces on an equilibrium of efficiency that requires flexibility. These are why economically competitive markets fail to achieve healthcare efficiency (Johansen & van den Bosch, 2017).
The concept of efficiency in health care has been described as Technical, Productive, and Allocative (Palmer & Torgerson, 1999). Extensive work has looked at special measures and populations for optimizing efficiency (Cylus & Papanicolas, 2016).
Efficient systems require predictable input, components, processes, and output, unlike efficiency in HCDS. The differences include:
- Biologic environments introduce variability in the system. Therefore, the HCDS efficiency will need to be flexible to diversity. Unfortunately, flexibility and efficiency counteract each other at industrial levels (Adler et al., 1999; AHRENS & CHAPMAN, 2004), and thus inefficiency is to be expected.
- Efficiency can be measured at two points:
- Efficiency of delivery
- Efficiency of outcome
Efficiency in HCDS means providing the most cost-efficient healthcare to those in need. As equity is a pillar of the HCDS, efficiency and equity are opposing forces (Guinness et al., 2011). Therefore, it is critical to have the broader determinants of health into consideration on HCDS. This broad spectrum of variables, individual level, and upstream factors (Dahlgren G & Whitehead M, 1991) will affect efficiency models applicable in one setting for a given population and inefficient in another (Hussey et al., 2009).
Healthcare Market:
The principle of maximizing profits applies to the four market types[1][2]. However, healthcare markets achieve Social Efficiency[3] and not economic efficiency (Folland & Goodman, 2013). This is due to Asymmetry of the information, Adverse selection, Moral hazard, Independent supply and demand stresses, and Externalities (Mwachofi & Al-Assaf, 2011).
Examples of Market Failure
At the onset of the pandemic, most governments, WHO assumed the costs of COVID-19 vaccination as they became available. Social media has disseminated incorrect information on vaccines (Lin et al., 2020; Wajahat Hussain, 2020). The Asymmetry of the information (AOI) has resulted in a sizable portion of the eligible population not being vaccinated (Coe et al., 2021; Malik et al., 2020). HCDS’s failure is a public relations problem and a breakdown in the trust of institutions (Soares et al., 2021).
Adverse selection (AS) compounds the AOI. There have been pockets of efficiency in vaccination with no equity for the world population (Mathieu et al., 2021).
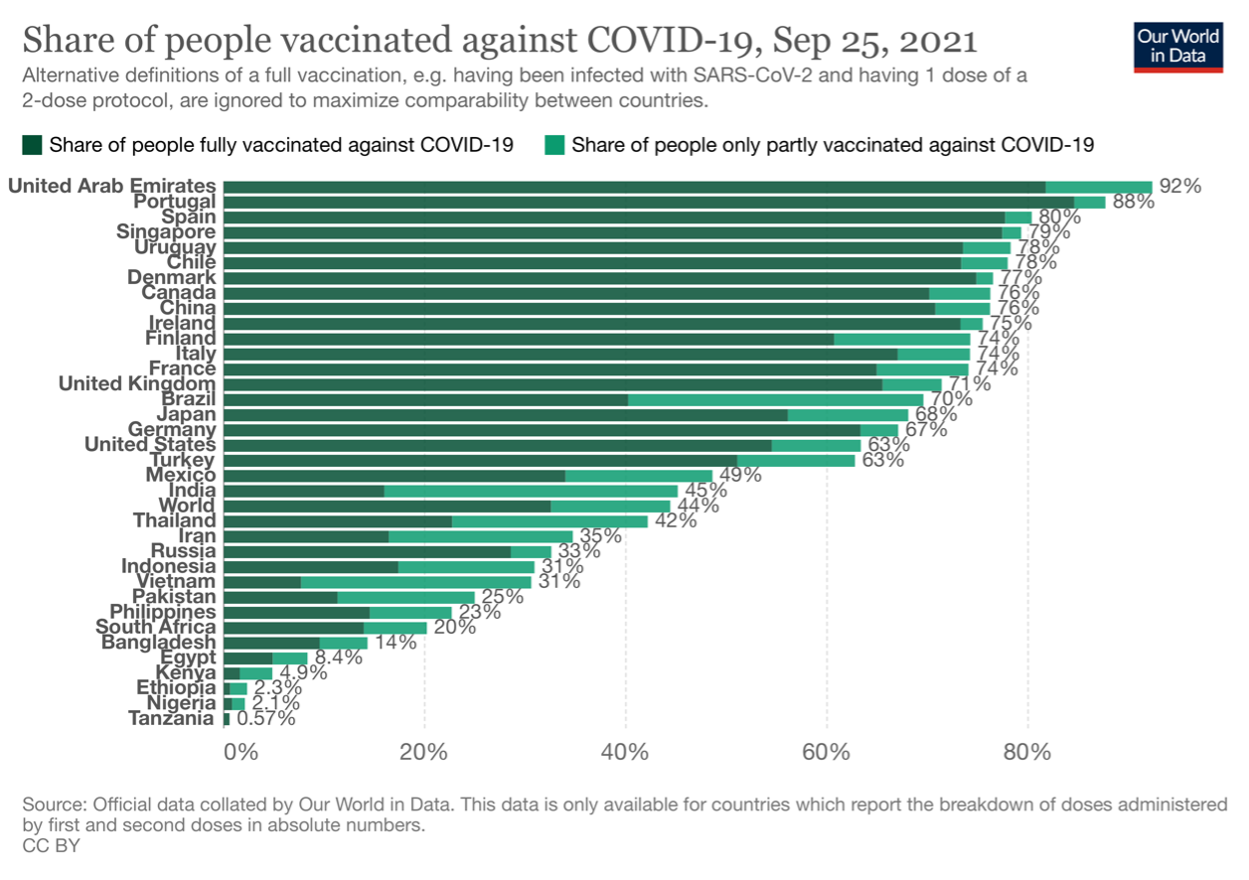 This is due to the AOI and the structural inequities in HCDS (Hyder et al., 2021). Few countries are offering vaccine boosters, where most of the world’s population has not received any.
This is due to the AOI and the structural inequities in HCDS (Hyder et al., 2021). Few countries are offering vaccine boosters, where most of the world’s population has not received any.
References:
Adler, P. S., Goldoftas, B., & Levine, D. I. (1999). Flexibility Versus Efficiency? A Case Study of Model Changeovers in the Toyota Production System. Organization Science, 10(1), 43–68. https://doi.org/10.1287/orsc.10.1.43
Adler, P. S., Goldoftas, B., & Levine, D. I. (1999). Flexibility Versus Efficiency? A Case Study of Model Changeovers in the Toyota Production System. Organization Science, 10(1), 43–68. https://doi.org/10.1287/orsc.10.1.43
AHRENS, T., & CHAPMAN, C. S. (2004). Accounting for Flexibility and Efficiency: A Field Study of Management Control Systems in a Restaurant Chain*. Contemporary Accounting Research, 21(2), 271–301. https://doi.org/https://doi.org/10.1506/VJR6-RP75-7GUX-XH0X
Coe, A. B., Elliott, M. H., Gatewood, S. B. S., Goode, J. V. R., & Moczygemba, L. R. (2021). Perceptions and predictors of intention to receive the COVID-19 vaccine. Research in Social and Administrative Pharmacy. https://doi.org/10.1016/j.sapharm.2021.04.023
Cylus, J., & Papanicolas, I. (2016). Health System Efficiency 46 How to make measurement matter for policy and management. London.
Dahlgren G, & Whitehead M. (1991). Dahlgren and Whitehead (1991) – Policies and strategies to promote social equity in health. Stockholm: Institute for future studies. Dahlgren G, Whitehead M. Retrieved from https://core.ac.uk/display/6472456
Enrique, B., & Marta, B. (2020). Efficacy, Effectiveness and Efficiency in the Health Care: The Need for an Agreement to Clarify its Meaning. International Archives of Public Health and Community Medicine, 4(1). https://doi.org/10.23937/2643-4512/1710035
Folland, S., & Goodman, A. (2013). The Economics of Health and Health Care. Oakland: Pearson.
Guinness, L., Wiseman, V., & Wonderling, D. (2011). Introduction to health economics. (2nd ed. /). Maidenhead: McGraw-Hill/Open University Press.
Hussey, P. S., de Vries, H., Romley, J., Wang, M. C., Chen, S. S., Shekelle, P. G., & McGlynn, E. A. (2009). A systematic review of health care efficiency measures. Health Services Research, 44(3), 784–805. https://doi.org/10.1111/j.1475-6773.2008.00942.x
Hyder, A. A., Hyder, M. A., Nasir, K., & Ndebele, P. (2021). Inequitable COVID-19 vaccine distribution and its effects. Bulletin of the World Health Organization, 99(6), 406-406A. https://doi.org/10.2471/BLT.21.285616
Johansen, F., & van den Bosch, S. (2017). The scaling-up of Neighbourhood Care: From experiment towards a transformative movement in healthcare. Futures, 89, 60–73. https://doi.org/https://doi.org/10.1016/j.futures.2017.04.004
Lin, C. Y., Broström, A., Griffiths, M. D., & Pakpour, A. H. (2020). Investigating mediated effects of fear of COVID-19 and COVID-19 misunderstanding in the association between problematic social media use, psychological distress, and insomnia. Internet Interventions, 21. https://doi.org/10.1016/j.invent.2020.100345
Malik, A. A., McFadden, S. A. M., Elharake, J., & Omer, S. B. (2020). Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine, 26. https://doi.org/10.1016/j.eclinm.2020.100495
Mathieu, E., Ritchie, H., Ortiz-Ospina, E., Roser, M., Hasell, J., Appel, C., … Rodés-Guirao, L. (2021). A global database of COVID-19 vaccinations. Nature Human Behaviour, 5(7), 947–953. https://doi.org/10.1038/s41562-021-01122-8
Mills, A., & Gilson, L. (2009). Health Economics for Developing Countries: A Survival Kit. Esocialsciences.Com, Working Papers.
Mwachofi, A., & Al-Assaf, A. F. (2011). Health care market deviations from the ideal market. Sultan Qaboos University Medical Journal, 11(3), 328–337. Retrieved from https://pubmed.ncbi.nlm.nih.gov/22087373
Palmer, S., & Torgerson, D. J. (1999). Economic notes: definitions of efficiency. BMJ (Clinical Research Ed.), 318(7191), 1136. https://doi.org/10.1136/bmj.318.7191.1136
Petrou, A. (2014). Economic Efficiency. In A. C. Michalos (Ed.), Encyclopedia of Quality of Life and Well-Being Research (pp. 1793–1794). Dordrecht: Springer Netherlands. https://doi.org/10.1007/978-94-007-0753-5_818
Soares, P., Rocha, J. V., Moniz, M., Gama, A., Laires, P. A., Pedro, A. R., … Nunes, C. (2021). Factors associated with COVID-19 vaccine hesitancy. Vaccines, 9(3). https://doi.org/10.3390/vaccines9030300
Wajahat Hussain. (2020). Role of Social Media in COVID-19 Pandemic. The International Journal of Frontier Sciences, 4(2), 59–60. https://doi.org/10.37978/tijfs.v4i2.144
[1] Perfect competition, Monopoly, Oligopoly, Monopolistic competition
[2] Control of Total revenue (TR) and Cost (TC) to maximize profit
[3] An equilibrium point (Pareto Optimality) where Social Marginal Benefit (SMB) and the Cost (SMC) are equal
Medication Accumulation in Gut Bacteria May Curb Drug Effectiveness, Alter Gut Microbiome
October 05, 2021 2:06 pm
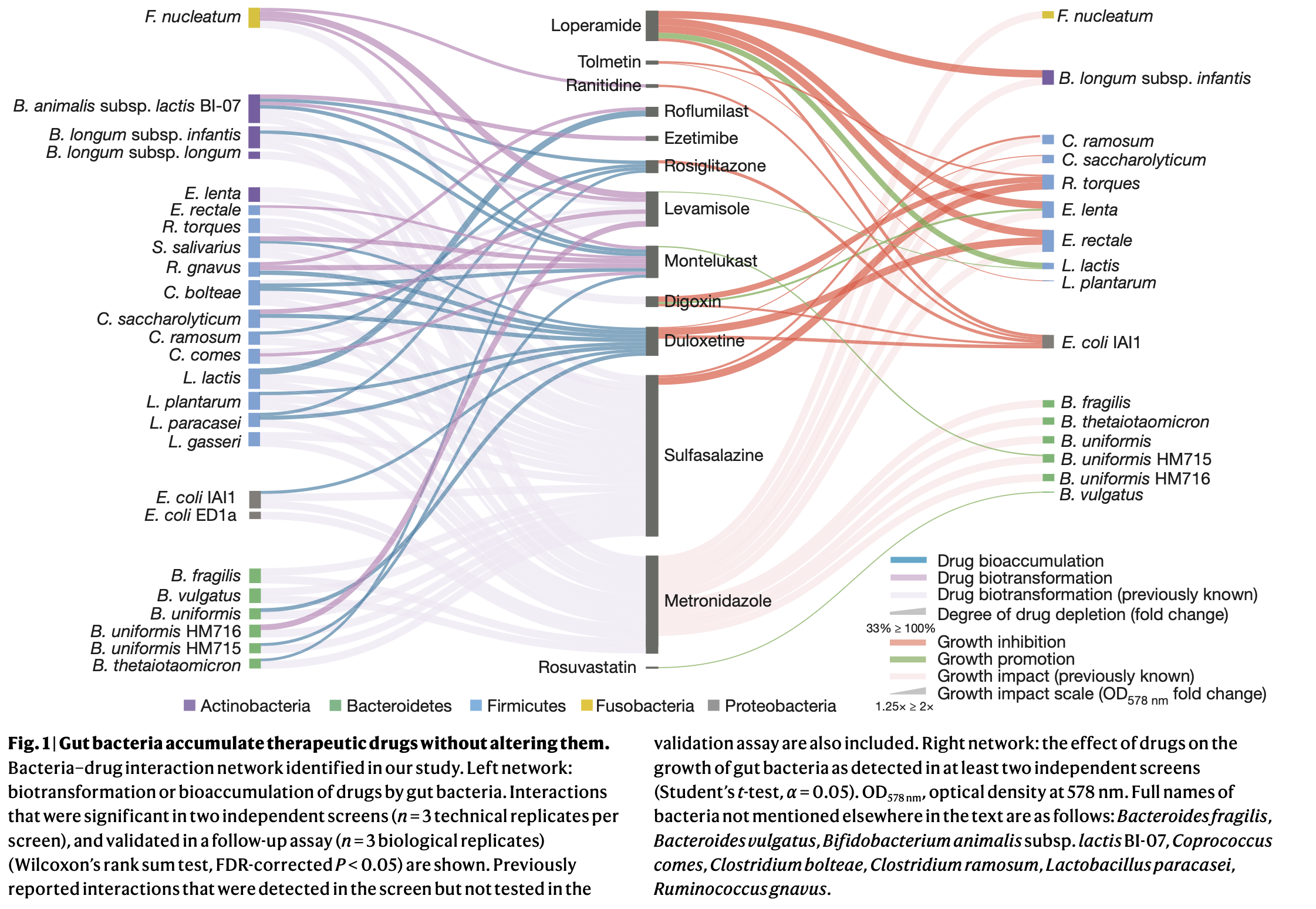 “As the authors note,” she said, “this study in bacterial isolates is only the first step towards understanding how bioaccumulation might influence drug metabolism and microbial community composition in the context of the far more complicated communities of microbes in the human body.”
“As the authors note,” she said, “this study in bacterial isolates is only the first step towards understanding how bioaccumulation might influence drug metabolism and microbial community composition in the context of the far more complicated communities of microbes in the human body.”
What’s New With the Nutrition Facts Label?
December 07, 2020 10:28 pm
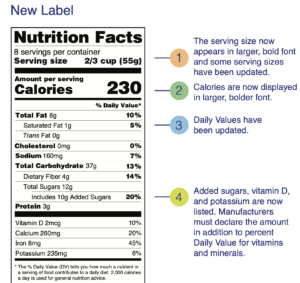
Get the Facts on Serving Size
December 07, 2020 9:57 pm
The New and Improved Nutrition Facts Label – Key Changes
December 07, 2020 9:53 pm
100% Fruit Juices and Risk of Cancer
April 16, 2020 8:54 pm
We have talked about the excess free calorie that is present with fruit juices. Now there is proven research article demonstrating the connection between surgary drinks and the increased risk of cancer. This study 
This study is significant for a number of reasons: It is a very large study with over a 100,000 subjects studied. Furthermore, it was specifically looking for association between nutrition and health.
The conclusion of this research article is self explanatory. Eliminating or cutting down high sugary drinks is an easy way of reducing cancer risk factors. The study also states that there were no identifiable association between the artificial sweeteners and cancer risks. However, this conclusion was not statistically significant. The relationship between sweeteners and cancer have been studied extensively in the past and we’ve shared several of them.
Length of Bowel : Hess or No Hess
March 22, 2020 5:58 pm
“…What is the length of my common channel” is probably one of the frequently asked questions about the duodenal switch operation in the office. This usually comes up at the initial consult when patients repost credible sources such as Dr. Google and Dr. Facebook for patient with different bowel length have done well or not so after duodenal switch operation. Dr. Hess described the Duodenal Switch by using total bowel length measurements and creating the common channel as a percentage of the total small bowel length. However, it seems that this is being done less and less.
This leads to my explanation that is on the website
Hess calculator : Bowel Length Calculator
How the actual measurements matters: Bowel length video link
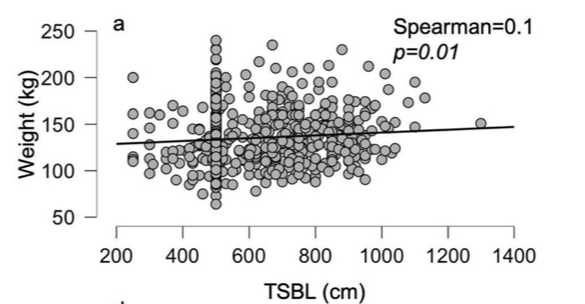
In 2019, Bekheit et.al published a very interesting study comparing total small bowel length (TSBL) to a number of variables such as height, weight, sex and BMI. They identified a few loose correlations. Male patient have longer TBSL than females. There was correlation between TSBL and height stronger in males than females but not statistically significant.
In Conclusion they reported ” Despite statistical significance of the correlation between the TSBL and the height and weight of the included participants, the correlation seems to have no clinical meaning since the effect size is negligible. ”
As I have previously discussed this Making the common and alimentary length standard for every duodenal switch patient will make some loose too much and other not enough weight.
Figure 1 shows TSBL on the horizontal axis, and height, weight, BMI and Age on the vertical axis. For the most part what they all show is that one can not predict how long a patients bowel is by any of the measures that we take in the office as a part of the routine exam.
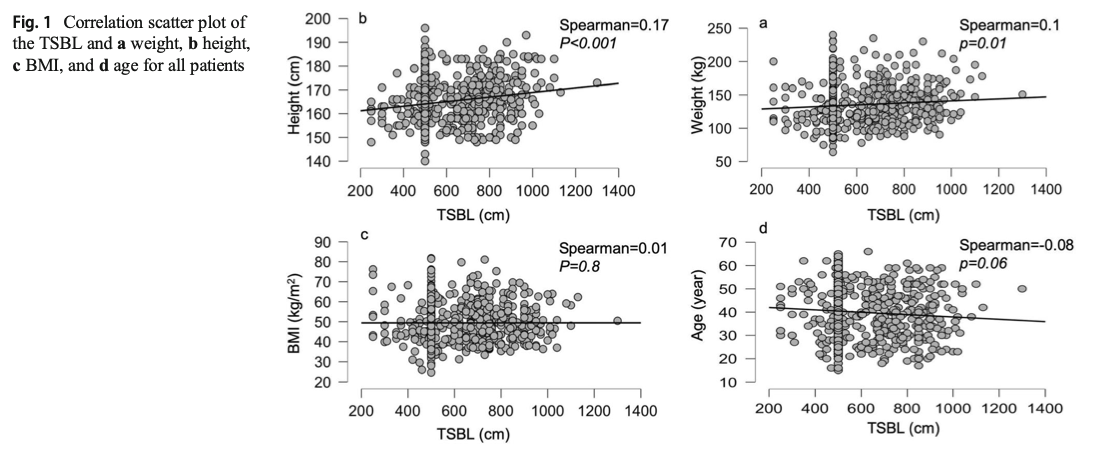
This raises, the concerns that I had raised previously. How could two similar patients who have the same weight, age, sex and BMI have the same surgery and expect the same result if one of them has TSBL of 400 cm and the other one 800cm?
 If both of the patients get the same “cookie cutter” duodenal switch with the same lengths, then the patient with TSBL of 400 will have much longer common channel if the surgeon does not customize the length of the bowel. This is an example of many patients whom we have revised over the years where they had a duodenal switch done with the “standard” 125cm common channel and when we measured the total length the patient had 500 cm TSBL.
If both of the patients get the same “cookie cutter” duodenal switch with the same lengths, then the patient with TSBL of 400 will have much longer common channel if the surgeon does not customize the length of the bowel. This is an example of many patients whom we have revised over the years where they had a duodenal switch done with the “standard” 125cm common channel and when we measured the total length the patient had 500 cm TSBL.
Protein Intake
October 14, 2019 7:08 am
Protein intake requirements change over time following weight loss surgery. This is based on the requirements imposed on our body by a number of variables. These include, activity level, muscle mass, over all health condition to name a few.
A very young muscular athletic male with a BMI or 30 will require much higher protein intake (and absorption) that an inactive older Female with the same BMI. The same young athletic male will require much higher protein intake is he is recovering from a surgery than his baseline.
As we have stated in the past, the protein intake, should be adequate and not excessive. High level of protein intake that are not accounted for based on muscle mass and activity level, will eventually result in weight gain. The best measure of protein intake in a stable weight patient over 3-4 years post op is their albumin and protein level. Following your yearly laboratory values at a minimum is an important part of weight loss surgery follow up care.
You also need to adjust protein intake when necessary. Protein needs increase depending on physical needs, infection, healing, pregnancy, surgery, age, injury, etc. Plastic surgery requires higher protein needs for appropriate healing.
Information on protein sources and quality here.
The basic formula for protein intake is 1gm/kg of ideal body weight. The calculator below will provide a guide for the protein into based on your stable weight in lbs.
Flagyl
September 25, 2019 9:07 am
Flagyl is sometimes prescribed for excessive gas and diarrhea. It is an antibiotics that works well on certain bacteria that accumulates in the GI tract and contributes to the gas and the bloating.
These bad bacteria flourish when patients consume significant and excessive fiber and carbohydrates (sugars, salad, pasta etc.) The FIRST line of defense against flatulence, bloating, and diarrhea should be eleminating the culprits in the diet. This point can not be stressed enough. Adding a daily dose of yogurt may improve symptoms due to yogurts probiotic benefits. To be beneficial, Yogurt should contain live bacteria cultures, not contain artificial sweeteners or have a high sugar content.
Artificial sweetness also area source of the excessive gas and should be avoided.
The Flagyl eliminates and reduces the bad bacteria. Along with a Probiotic and healthy dietary choices Flagyl can help to significantly improved or eliminate those symptoms of gas and diarrhea.
Before Flagyl is prescribed, it is important that the diet is critically examined to make sure that the carbohydrates and the fiber as source of gas and bloating is minimized or eliminated. Excessive use of medications that may be needed for other infections should be avoided.
Chronic diarrhea should be evaluated to rule out GI infection with C. diff bacteria or other bacteria or parasite.
Additional Information on C. Diff (Clostridium Difficile) and probiotics.