
Category: BPD/DS
Stapled Anastomosis
December 30, 2019 11:23 am
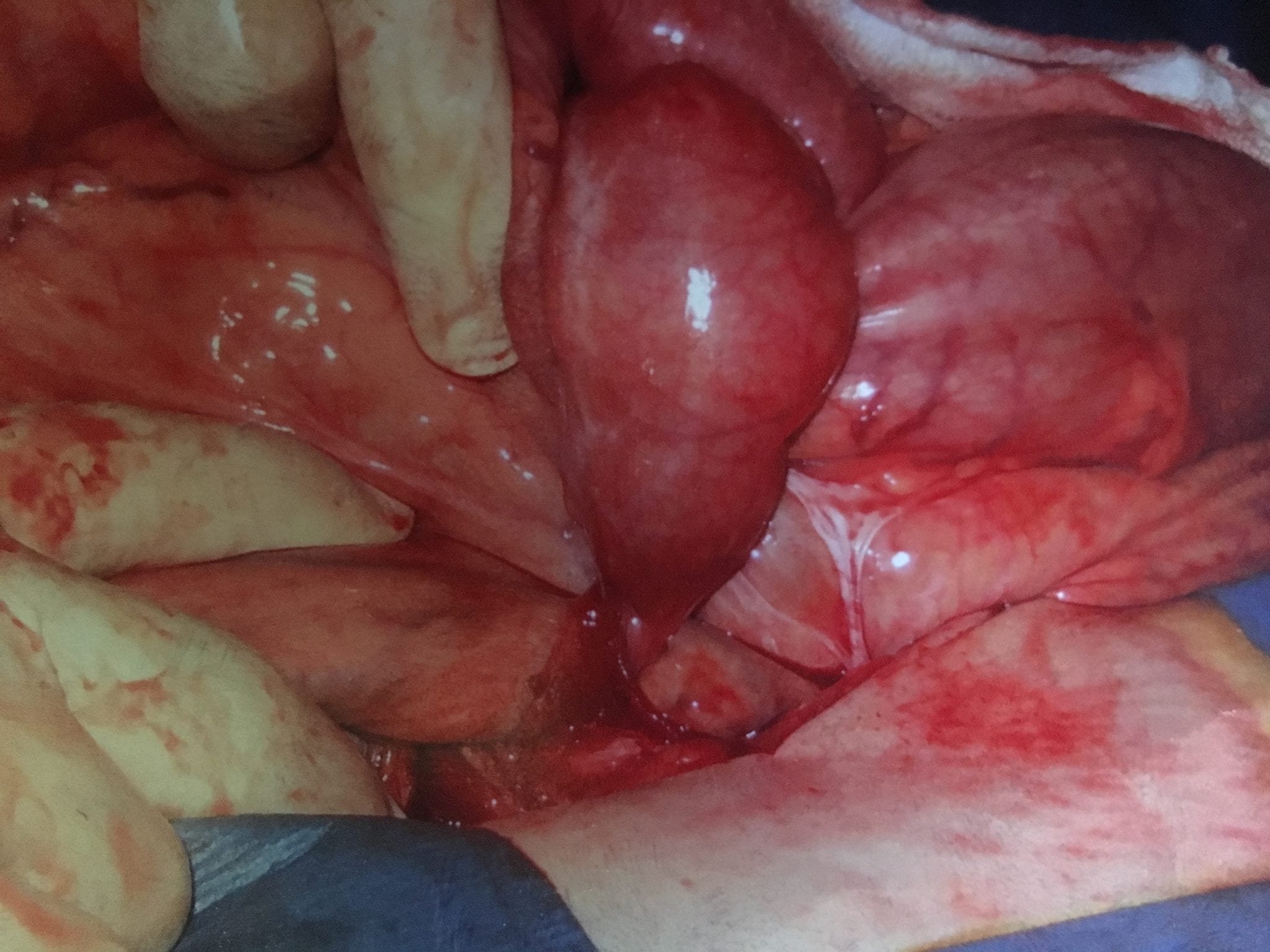
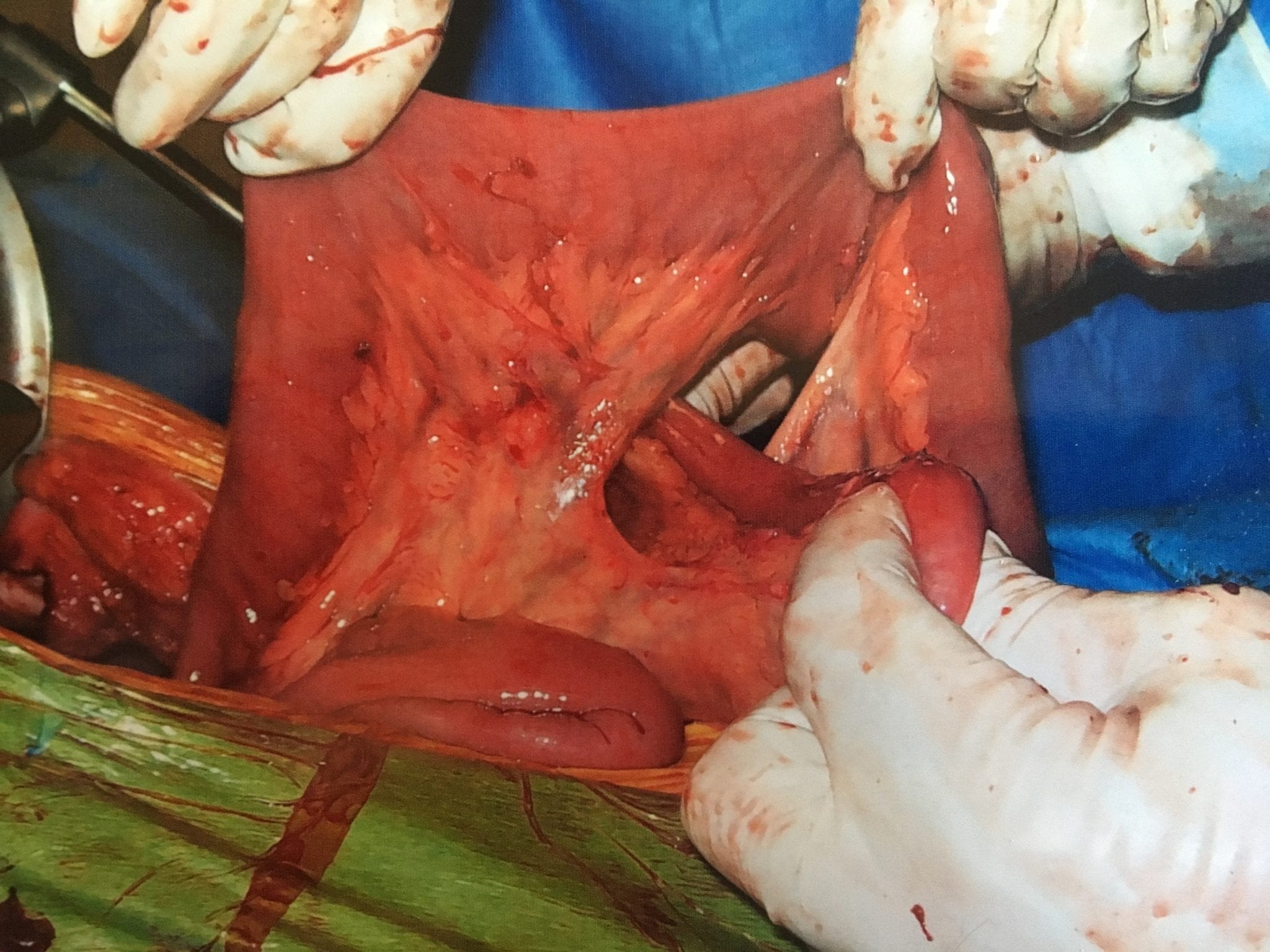
As I was looking over old archives, I came across the following pictures that were taken years ago. These were photographs taken to demonstrate the technique for the construction of the anastomosis of the biliopancreatic channel and alimentary channel of the Duodenal Switch.
The steps of doing the stapled anastomosis of the Duodenal Switch is generally unchanged during the laparoscopic approach to the procedure.
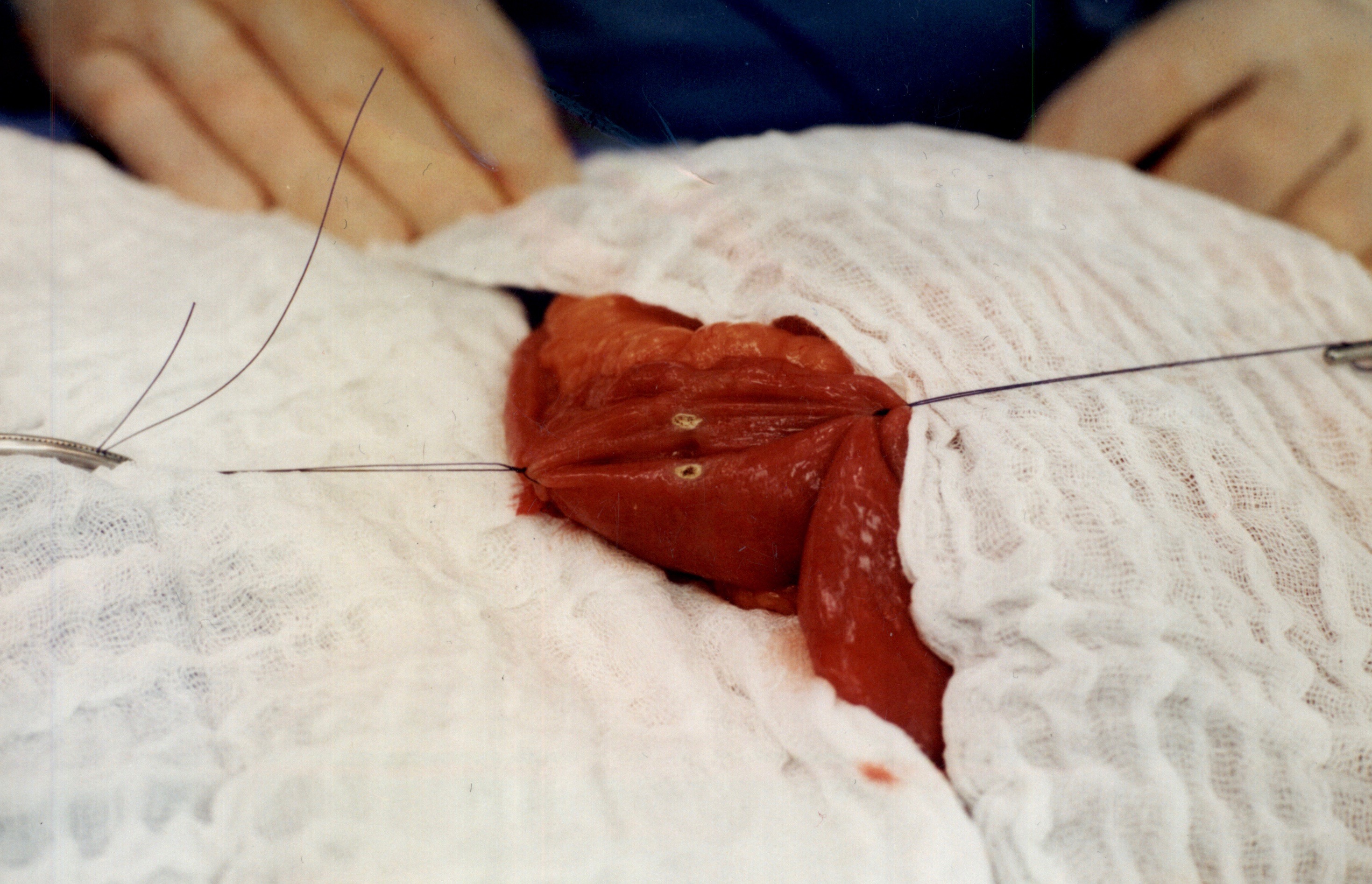
The stitches are placed to secure the bowel together. Two small openings are made in each limb of the bowel to be stapled together (the biliopancreatic limb on the bottom and the alimentary on the top of the image).
It is important to also align the bowel in the same peristalsis direction. This means that the contraction and the relaxation motion of the bowel should all point in the same direction. This should reduce the risk of complications such as intussusception.
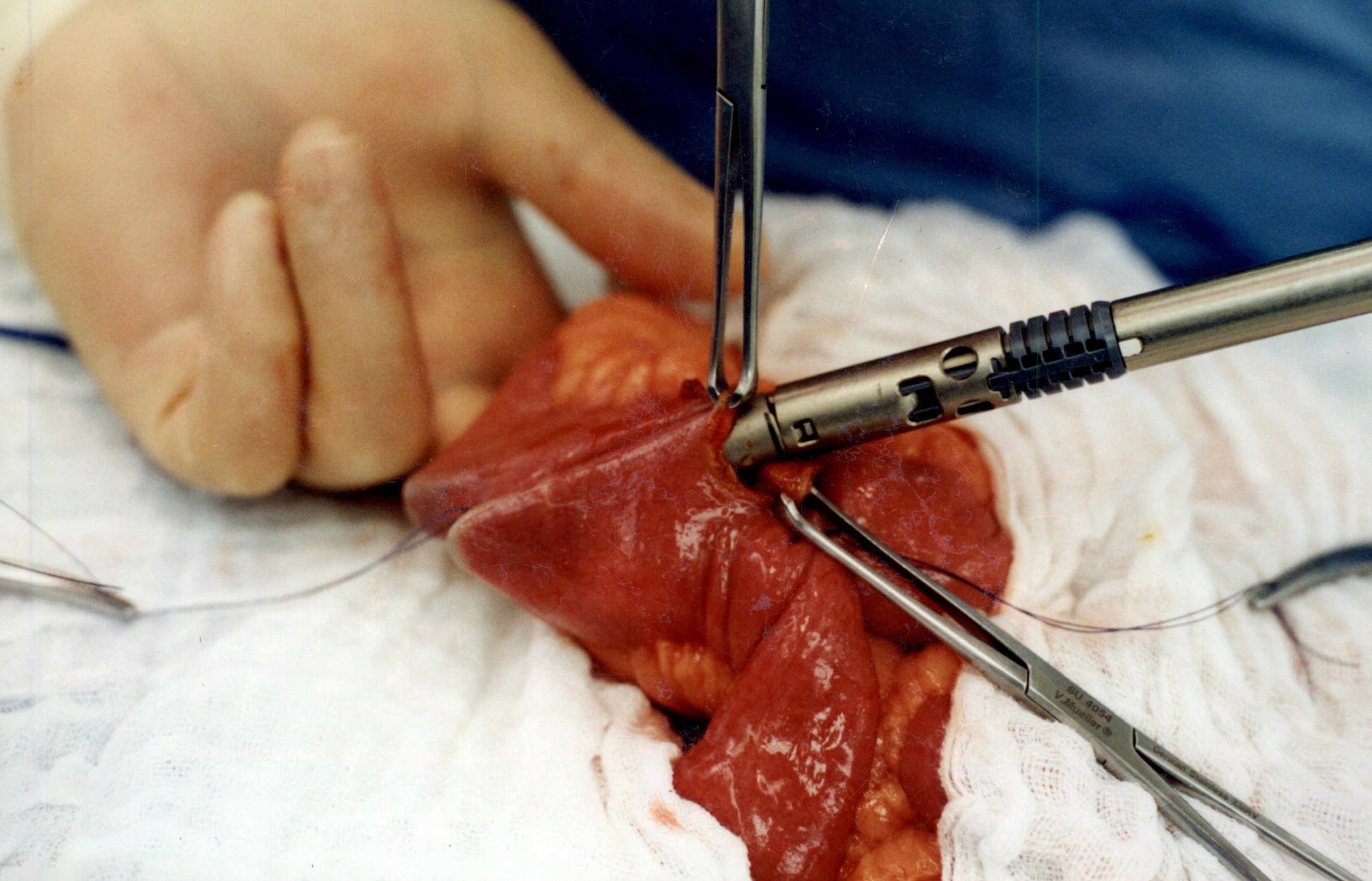
When the stapler is fired in opposite direction, a very wide anastomosis is created.
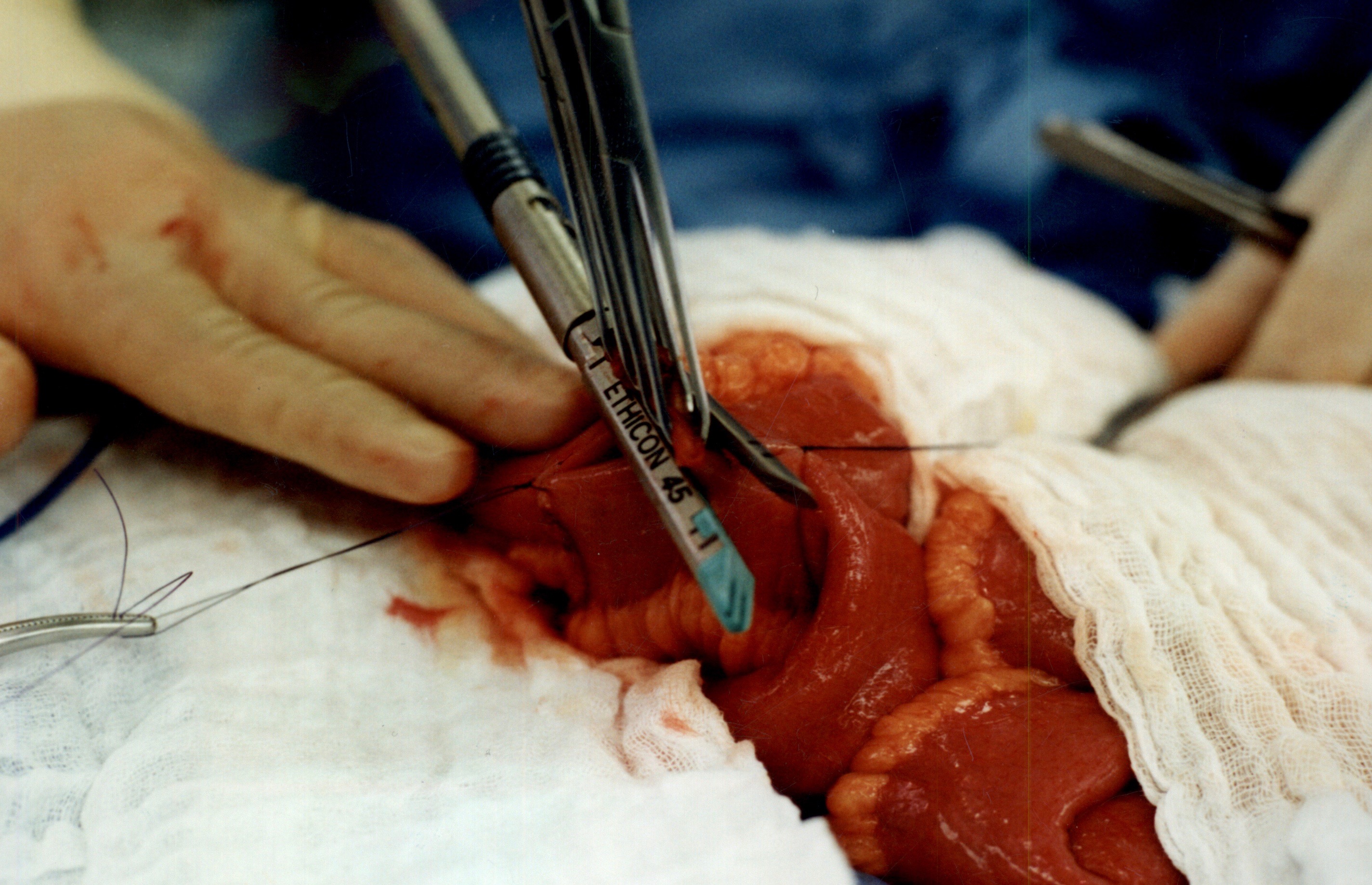
Once the anastomosis is created, then the last staple is used to close the opening that was made. This staple line is perpendicular to the direction of the anastomosis to avoid making the opening narrow.
We originally published this technique in 2003 on Obesity Surgery Journal.
Copper Deficiency Intravenous SupplementationExclusive Member Content
November 17, 2019 9:23 pm
Sleeve And Weight Regain
July 22, 2019 9:50 am
 Felsernreich et.al. demonstrated that 10 years after sleeve gastrectomy 33% were requiring revisions of their sleeve due to weight regain or reflux. 66% needed revision for weight loss and only 34% for reflux. Those patients who have revision to gastric bypass (in their practice all being revised with two exception) had resolution of their reflux however had no sustained weight loss after the revisions. This supports our position that we have had for years that the those patient who had the sleeve and are experiencing weight regain, recurrence of comorbidities inadequate weight loss ahould all be revised to the duodenal switch operation.
Felsernreich et.al. demonstrated that 10 years after sleeve gastrectomy 33% were requiring revisions of their sleeve due to weight regain or reflux. 66% needed revision for weight loss and only 34% for reflux. Those patients who have revision to gastric bypass (in their practice all being revised with two exception) had resolution of their reflux however had no sustained weight loss after the revisions. This supports our position that we have had for years that the those patient who had the sleeve and are experiencing weight regain, recurrence of comorbidities inadequate weight loss ahould all be revised to the duodenal switch operation. 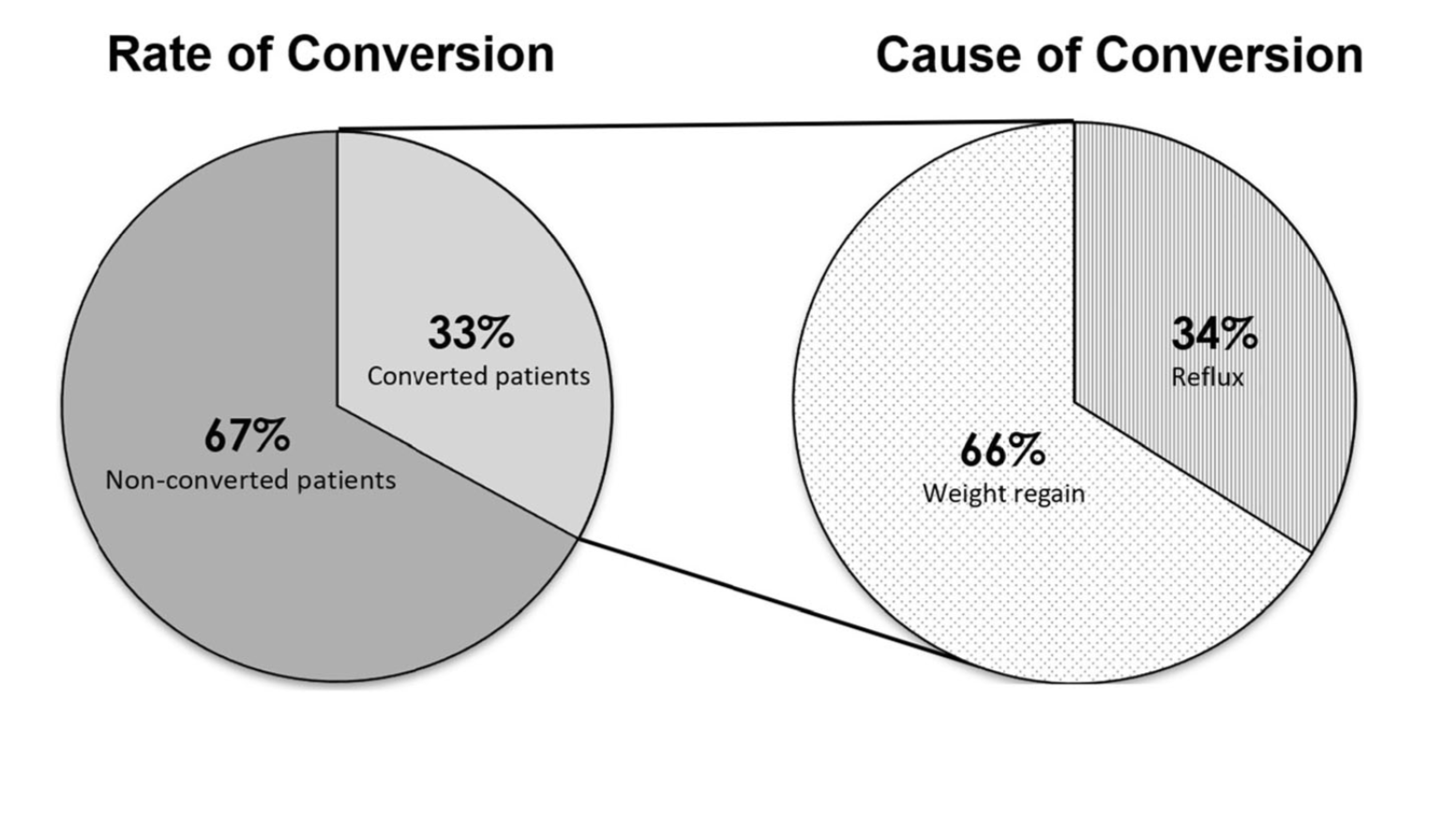
Sunscreen
June 27, 2019 3:03 am
Recently there has been some research and concern regarding sunscreen and the chemicals within them. This has led to findings that can be concerning but that need further research.
Post weight loss surgical patients, and in general patients who suffer with obesity, before or after weight loss surgery, have low vitamin D level. This may be caused by a number of factors. One such factor may be the reluctance to get skin exposed to sunlight in order for the bodies natural Vitamin D pathways functioning.
The recommendations are for daily exposure to sun. This not only is critical to the vitamin D metabolic pathways, but also help with bone health, immune function, mood, counteracting depression.
In a recently published online article, concerns were raised that some of the ingredients of some of few sunscreens are absorbed in the blood stream. This is a small study, and as the results indicates, it is not recommending to stop using the sun screens. Be aware of your sun exposure, timing exposure, and the ingredients in your sunscreen.
You can find past blog posts on Vitamin D, Bone health, etc here
Thyroid Medication Absorption And Weight Loss Surgery
June 10, 2019 8:59 am
Question : “Do I have to take higher dose of thyroid medication after the duodenal switch? ”
Answer : “Maybe”
With all weight loss surgical procedures, there may be changes to absorption of medications. It is easily understood why duodenal switch may results in decreased absorption of fat-soluble medication. What is not as clear is the reduction in absorption of other medication with procedures that do not explicitly change the absorption at the level of the small bowel directly.
The research data is all over on this topic. There is published literature that shows improvement in the thyroid function after gastric bypass and the sleeve gastrectomy. However, the exact mechanism is not completely understood.
There is research that reports “…decreased postoperative levothyroxine requirements.” Other have shows no correlation between the length of the bowel distal to duodenum to absorption of thyroid medication.
With all this confusing data, the best course would be to always “treat the patient and not the lab results.”
 If a patients who has been on medications with stable number and symptoms, suddenly presents with complaints of hypothyroidism after weight loss surgery, it’s possible the medications should be up adjusted even if the thyroid lab values may not be as defining.
If a patients who has been on medications with stable number and symptoms, suddenly presents with complaints of hypothyroidism after weight loss surgery, it’s possible the medications should be up adjusted even if the thyroid lab values may not be as defining.
Osteoporosis Medications, Action and Side Effects
May 25, 2019 3:40 pm
Treatment options should be approached is a global and systemic fashion. It is critical that the nutritional status is at its best possible and optimized for important healthy bone vitamins and minerals. Low protein needs to be corrected. Special attention should be given to nutrients, minerals and vitamins. These include Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1/K2to name a few.
Healthy bones require ongoing and routine force in the form of exercise to remain health. Just as exercise improves muscle strength, it also improves bone health. Exercise is also critical in improving bone structure and density. Ideally, exercise should be weight bearing and resistance. Examples include: hiking, walking, jogging, climbing stairs, playing tennis, and dancing. Resistance type exercise is weight lifting and resistance bands. These exercise work by creating a pull or force on the bone either by gravity, movement or weight. Always check with your physician before beginning an exercise routine, start slowly and building up to longer periods of time. The ideal goal would be at least 30 minutes a day, every day, if you are able.
We frequently see patients immediately started on osteoporosis medications without checking or improving some of the nutritional markers noted above or without looking at exercise history. In some case, the medication recommended are contraindicated due to nutritional status.
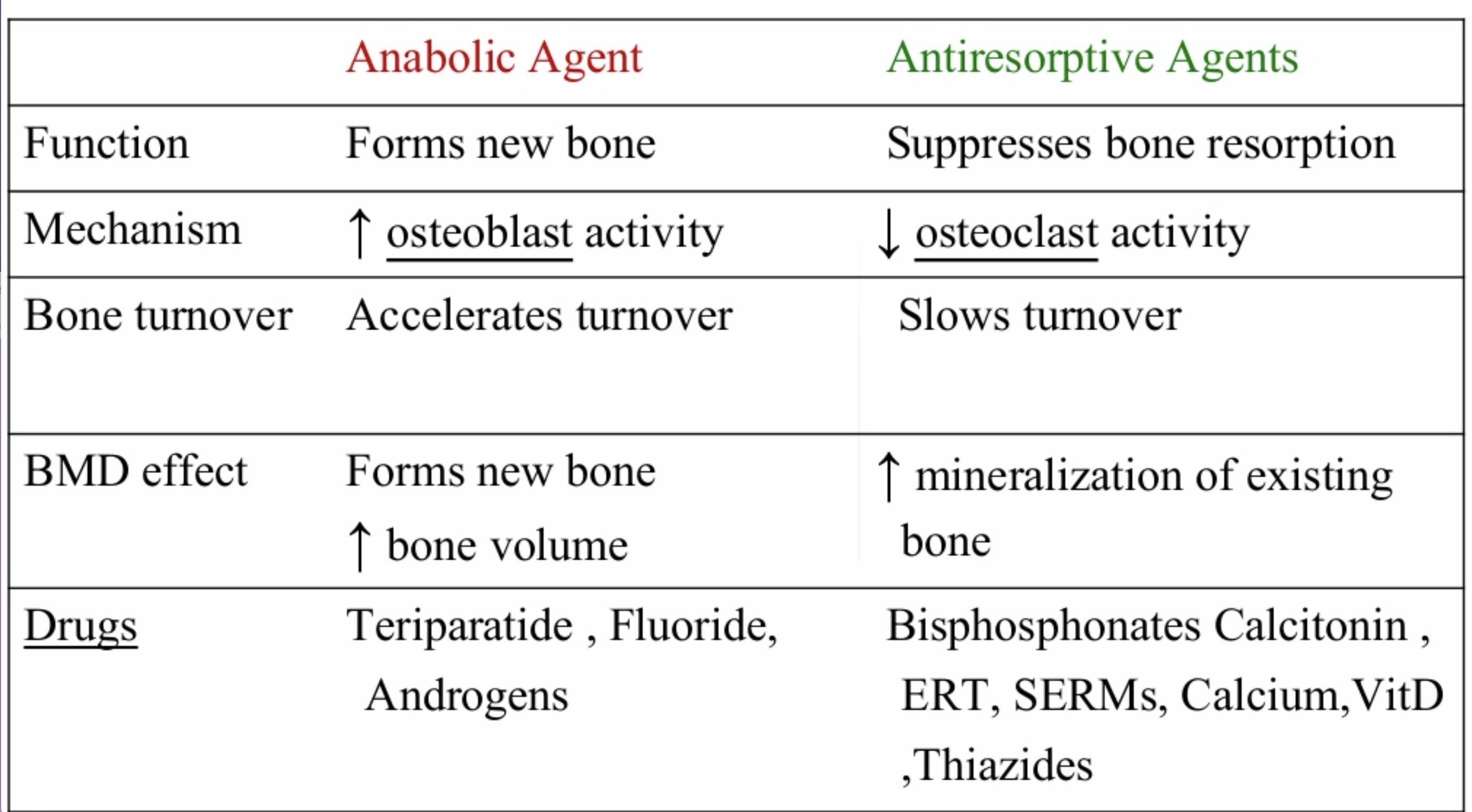
The medications can be grouped in to those that help with new bone formation (Anabolic agents) or those that help by suppressing the bone breakdown phase (Antiresorptive agents).
National Osteoporosis Foundation has an exhaustive list (below) of medications for treatment of Osteoporosis.
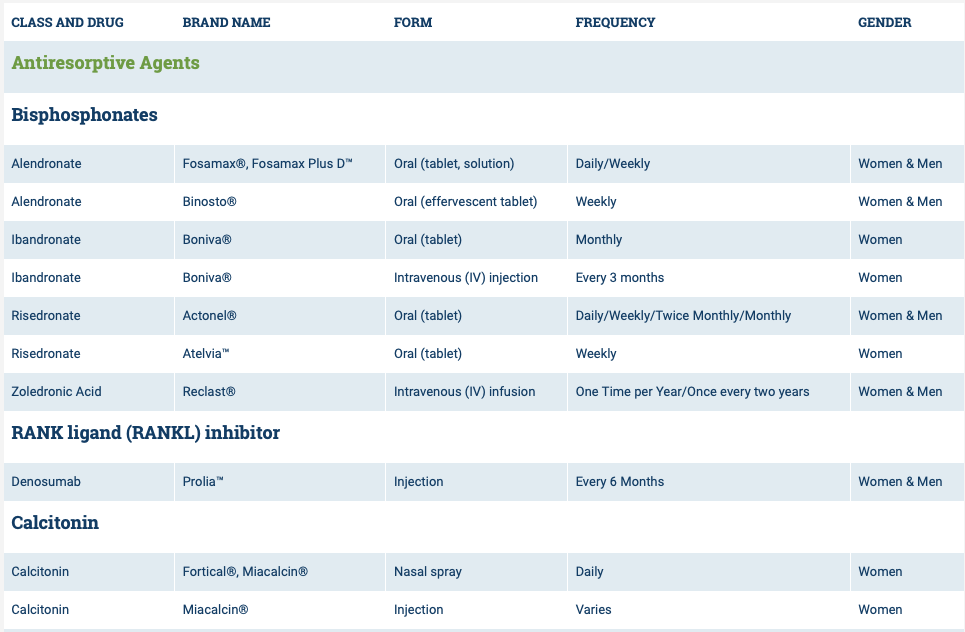

The table below outlines the side effects and mechanism of the actions of the common medications used for treatment of osteoporosis which was published by the University Health News Publication on August of 2014.
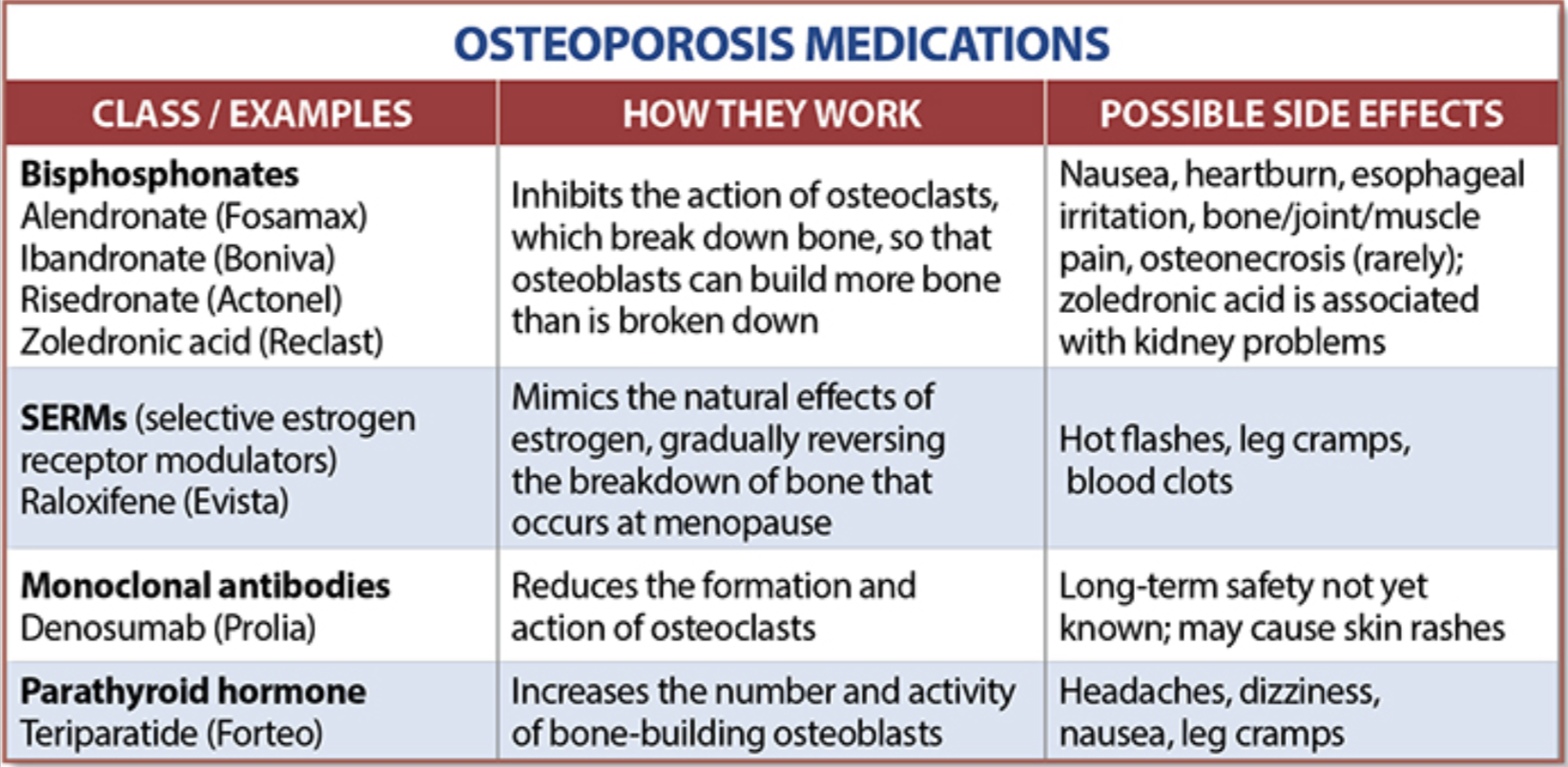
With all this information, the few points to remember is that the most important factors in healthy bone structure are the nutritional status Protein, Calcium, Magnesium, Vitamin D, and Vitamin K1 levels.
This is an animation of normal bone Metabolism. It shows how bone structures is taken down and rebuilt continuously. This allows for a healthy bone maintainence as we age. The key is the balance of breakdown (osteoclast) and the build up (osteoblast) activity is regulated. Osteoporosis develops when there is more breakdown that build up. 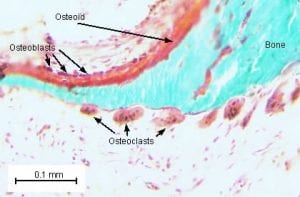
With permission of Dr. Susan Ott of University of Washington.
Additional information available on her site.
Past blogs on Bone Health.
Sleeve Gastrectomy Failure
May 07, 2019 12:53 pm
Sleeve gastrectomy (SG) is the most commons performed weight loss surgery in the US. There is a subset of patients for which Sleeve Gastrectomy will be inefficient/ineffective. Sleeve Gastrectomy failure may be defined as inadequate weight loss or weight regain. However, in some cases this may also include non resolution of some of the co-morbidities of obesity, and/or recurrence of others.
Biertho, et. al, (Surgery for Obesity and Related Diseases 14 (2018) 1570–1580) Published a study titled “Second-stage duodenal switch for sleeve gastrectomy failure: A matched controlled trial” where 118 patients were decided in two groups. One group had the duodenal switch as a singe procedure, and the second group had the sleeve gastrectomy followup by the second stage duodenal switch. They concluded that “Second-stage DS is an effective option for the management of suboptimal outcomes of SG, with an additional 41% excess weight loss and 35% remission rate for type 2 diabetes. At 3 years, the global outcomes of staged approach did not significantly differ from single-stage BPD-DS; however, longer-term outcomes are still needed.”
They showed that the remission rate of the obesity-related co-morbidities was improved.
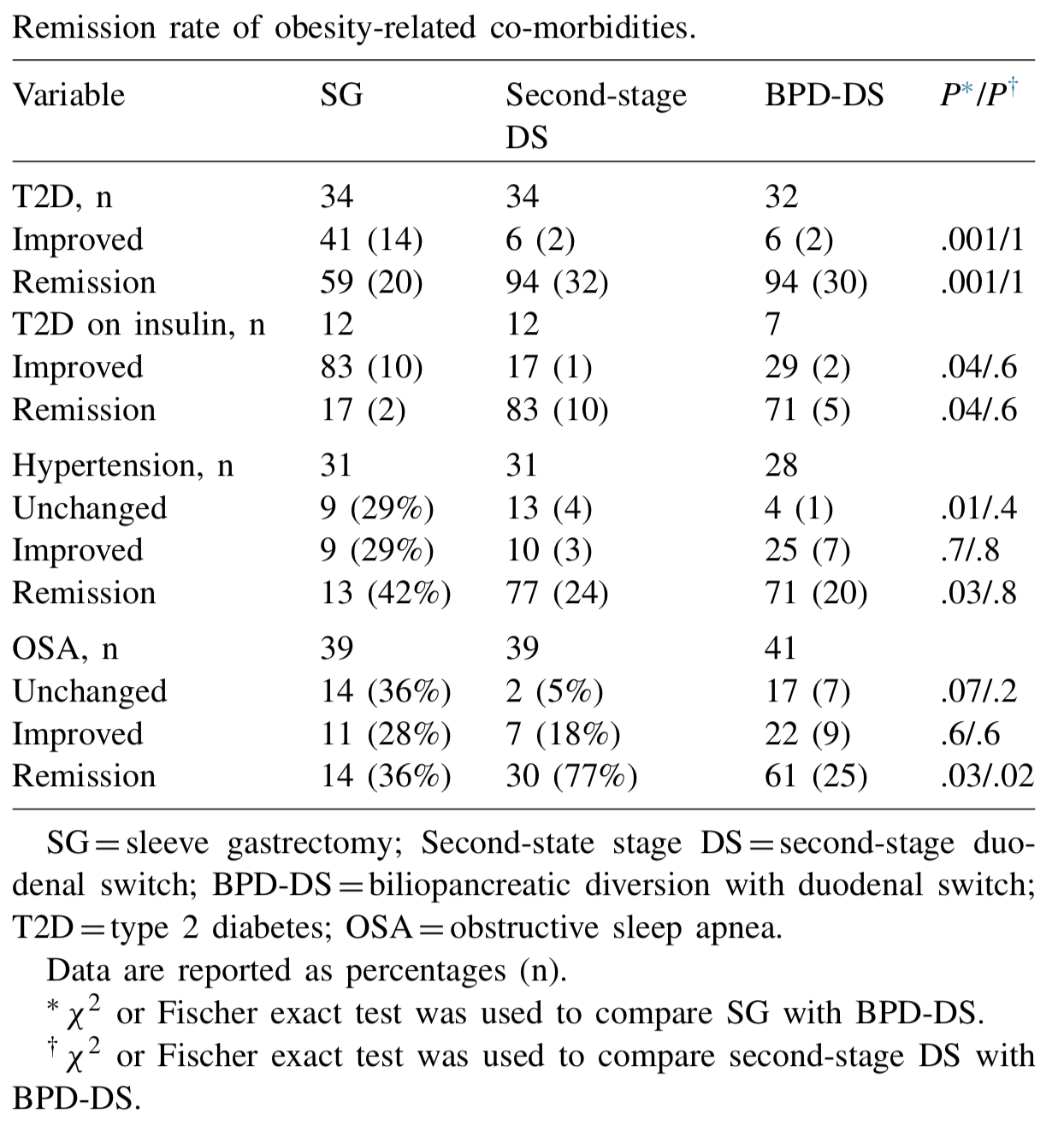
The weight loss rate that had stopped, or in some cases where weight gain had been noted, were both reversed where by at at average of 24 months after addition of the DS to the SG patients would experience additional 39% Mean excess weight loss. 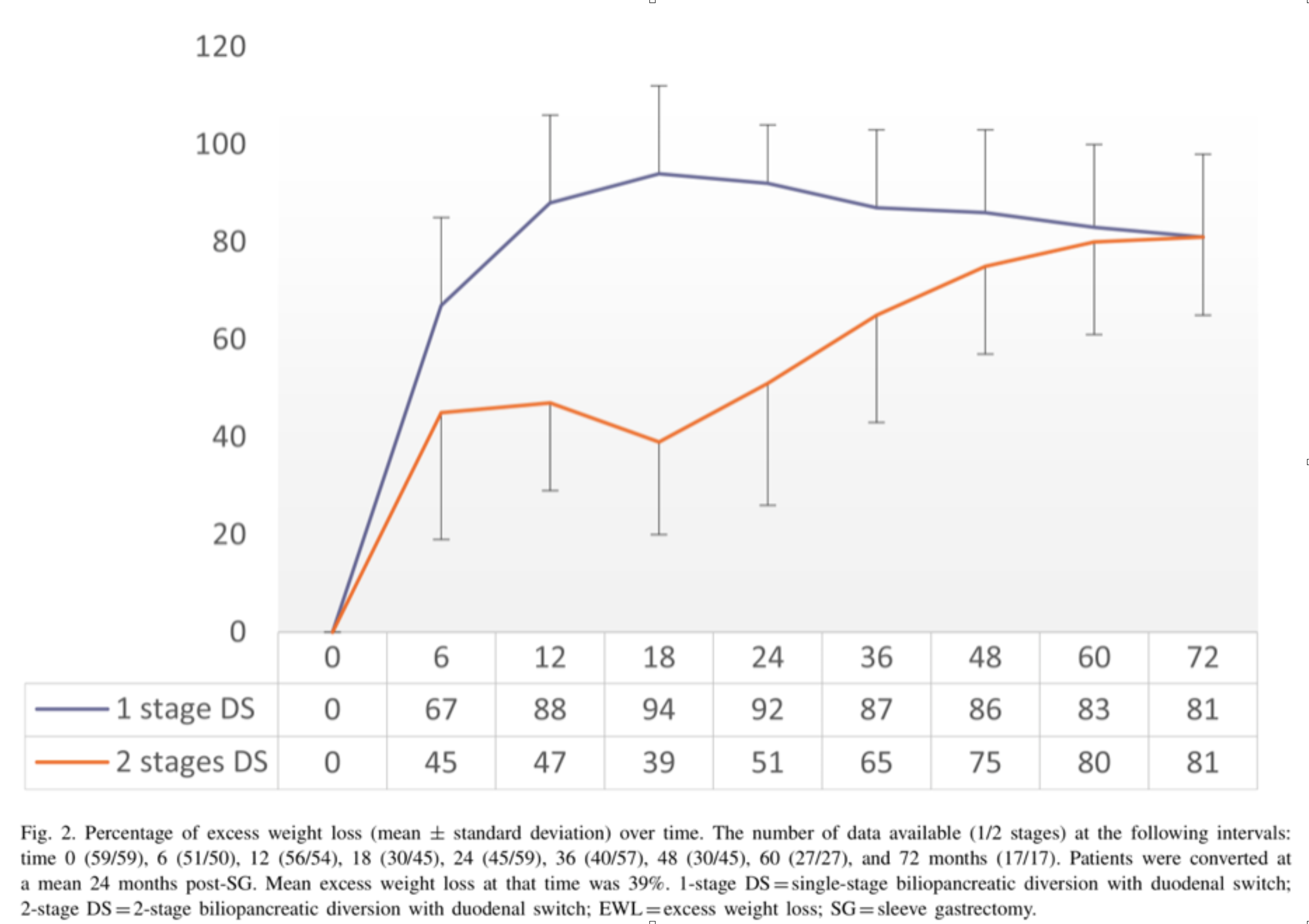
With regards to alternative approaches they indicate “ Other forms of revisions have been described, (i.e., adjustable or nonadjustable gastric band, plication, endoscopic balloon), with limited scientific evidence on their efficacy or safety. These procedures are mostly considered investigational and should be performed under Ethical Review Board approved protocols.”
In summary, patients may be offered a number of alternative if they are experiencing weight regain, inadequate weight loss, or return of co-morbidities after sleeve gastrectomy failure. We have seen a variety of them in our office. Patients who have had band placed on the sleeve, or are scheduled to have gastric balloons placed. As I have always said, buyers beware and know your outcomes and resolution of co-morbities.
Duodenal switch operation, (not the single anastomosis look alike) results in sustained weight loss and resolution of the co-morbidities. A second stage Duodenal Switch can mean adding the intestinal procedure to an existing Sleeve Gastrectomy. Some patients have required an adjustment to their Sleeve Gastrectomy in addition to adding the Duodenal Switch intestinal portion. Finding the right balance for each patient is a crucial part of our practice.
SIPS, SADI-S, Loop DS
May 01, 2019 9:03 am

The American Society for Metabolic and Bariatric Surgery (ASMBS) and MBSAQUIP-A on March of 2019, published and updated list of “Endorsed Procedures and Devices”
Endorsed Procedures and Devices | American Society for Metabolic and Bariatric Surgery
Note that any surgical procedures that does not employ two anastomosis, are not endorsed and are only recommended to be performed with an IRB (Institutional Review Board) or an IRB exemption. Duodenal Switch, Sleeve Gastrectomy, Roux en Y Gastric Bypass, Gastric Balloon, Adjustable Gastric Banding, and Nerve Blocking which are endorsed procedures.
SIPS, SADI-S, SIPS, Loop DS are all in the category of the “Non-Endorsed Procedures and Devices”. To see an anatomical comparison of these procedures to the Duodenal Switch procedure.
Patients should request that their consent be clearly defined and should explicitly outline the procedure that is being proposed to them. This is to avoid a patient having a procedure that they assumed, or are led to believe to be a Duodenal Switch operation with two anastomosis. Do your due diligence and know the procedure you want. Investigate if the surgeon you are working with performs the procedure you are interested in. Have them draw a picture of the procedure or give you a diagram of the procedure.
Dr. Facebook
March 22, 2019 8:24 am
We have become reliant on the information that we obtain from the internet, specifically platforms such as Facebook. In our practice we have to continuously correct information that patients have obtained from other patients, unmonitored sites, blogs, and postings. Most of this information is based on individual experiences that has become gospel. “Fat is good for you” is one of them. To clarify, some health fat (olive oil, avocado, Omega 3) is healthy and needed for all patients. We do not recommend “fat bombs” as a part of ones daily dietary intake.
The following article was written on the accuracy of nutritional posts in support groups on Facebook.
Koalall et. all in SAORD, December 2018 Volume 14, Issue 12, Pages 1897–1902 published
“Content and accuracy of nutrition-related posts in bariatric surgery Facebook support groups”
The conclusion, as suspected, that “Over half of the posts contained inaccurate content or information that was too ambiguous to determine accuracy..:”

It is our recommendation before any dietary recommendations are taken from facebook and the like, the source of the information should be verified. As I have stated in the past, a frequent flier passenger is probably not qualified to fly a
commercial airplane, any more than a previous weight loss surgical patient providing medical and nutritional advice. We realize that there is significant value to the forum for exchange of information and sharing of experiences with other weight loss surgical patients as long as the information is well sourced and verified.
Adhesions, Internal Hernia And Bowel Obstruction
December 15, 2018 2:35 pm
Adhesions are fibrous bands of scar tissue that form during the healing process. Following surgery, many people live normally with this scar tissue. However, they are also the cause of bowel obstruction when the adhesions form in such a way that causes a segment of the bowel to either get trapped, or form a “knot”. In both of those cases, the end result is a partial narrowing or a complete blockage of the intestines. This is called bowel obstruction.
Without treatment, the blocked parts of the intestine can die, leading to serious issues. However, with prompt medical care, intestinal obstruction often can be successfully treated.
Other causes of bowel obstruction:
- In children, the most common cause of intestinal obstruction is telescoping of the intestine (intussusception).
- Intussusception telescoping of the interstine
- Hernias — portions of intestine that protrude into another part of your body
- Inflammatory bowel diseases, such as Crohn’s disease
- Diverticulitis — a condition in which small, bulging pouches (diverticula) in the digestive tract become inflamed or infected
- Twisting of the colon (volvulus)
- Impacted feces
- Colon Cancer
In patients who haven’t Bariatric / weight loss surgery or an untouched GI track, bowel obstruction may manifest itself by symptoms of loss of appetite, constipation, nausea, vomiting, enlarged abdomen, abdominal pain, cramping, with no passage of gas or bowel movements.
However, patients who have had a weight loss surgery (Duodenal Switch, or the Gastric Bypass) because of the parallel limbs of the small bowel, the symptoms outlined above may not present. The diagnosis of a bowel obstruction, when suspected, should be identified with CT scan of the abdomen and pelvis with Oral and IV contrast. A CT scan with no oral contrast or water instead of oral contrast is inadequate and may lead to a delay in diagnosis and surgical intervention. Examples of Bowel Obstruction CT findings were discussed previously.
The treatment for an internal hernia and adhesions causing a bowel obstruction depending on the severity may range from observation to surgical intervention in order to release the small bowel from the constraints of the adhesions.