
Category: Bariatric surgery
A patient story: Lap Band complication and Wegovy
October 24, 2024 4:30 pm
Not too long ago, I saw an old patient who had seen me years ago after having had a lap band placed for weight loss. At the time, I recommended that the lap band be removed and that alternative plans be made. I suspected a slipped band. We discussed the reality that after the band removal, weight gain is to be expected. Several surgical options were discussed, and the patient dismissed them as “too radical.” The patient decided to “deal” with the ongoing nausea and vomiting since it was a small price to pay for the weight loss. I warned the patient that elective removal of the band is much safer than an emergency procedure in the middle of the night when it is least convenient. The patient did end up with an emergency lap band removal and was started on GLP-1 Agonists (Wegovy) because of the weight gain that followed the band removal. The side effects of the medication were debilitating, with nausea, dizziness, and fainting due to low blood sugar. The drug has all been stopped, and most, not all, of the side effects are resolved. The plan is to get this patient in a better shape and, reevaluate the esophagus and the stomach, and formulate a strategy based on the blood work, upper endoscopy, upper GI study findings and decide if the patient will be a good candidate for the Laparoscopic sleeve or the duodenal switch operation.
Here are my recommendations:
- Patients should avoid lap bands. Those with lap bands, regardless of how they feel and whether they are having issues with them, should have the lap band removed immediately before they end up in the emergency room or have irreversible changes to the cells or function of the stomach and esophagus.
- Patients who have the lap band removed will have less weight loss with the sleeve than those who have the sleeve as the primary procedure (the lesson here is that a less invasive, seemingly easy solution is much worse long term; more on this below). Lap Band patients should be revised to the duodenal switch, SPIS, SADI, or Gastric bypass if they have substantial weight to lose.
- GLP-1 agonist medication should be avoided. It is not a solution to the underlying problem but a band-aid covering the metabolic derangement.
- GLP-1 agonist medication needs to be taken long term, and there is no exit strategy– when the patients stop taking the drug, the weight comes back, in addition to the complication associated with it.
- I have also heard that “if it were bad, then the FDA would not approve it.” well, let’s think about it: the FDA approved the Lap band and Phen-Fen, and we all know how these worked out.
- There are no shortcuts, simple injections, or a pill for the complex, multifaceted condition of obesity. Advocating solutions with no long-term outcome, significant complications, and safety concerns is irresponsible.
- A diabetic patient should take the medication LIFELONG to control their blood sugars, including the GLP-1 agonist class of drugs. The concerns are for these medications being used for the treatment of obesity

Radiology film of normal position and a slipped LapBand
SUMMARY: Buyers beware- those who choose to embark on the dangerous load of GLP-1 agonist medications should be prepared to deal with the short and long-term complications of the medication and its withdrawal. This is like the problems that are being seen with patients who choose to have a lap band because it was advocated as simple, reversible, and the Phen fen medication for weight loss with the associated cardiac complication.
https://www.dssurgery.com/wp-content/uploads/2024/09/P000008S017b.pdf
https://www.dssurgery.com/wp-content/uploads/2024/09/20-year-all-procdure-metaanalysis.pdf
https://www.dssurgery.com/weight-loss-injection/
https://www.dssurgery.com/glp-1/
https://www.dssurgery.com/weight-loss-medications-compared-to-surgery/
https://www.dssurgery.com/articles/glp-1-agonists-a…agency-clinicians/
https://www.dssurgery.com/articles/managing-the-gas…clinical-practice/Survey
December 16, 2023 9:54 am
Covid 19:Anesthesia, Weight Loss Surgery and Malnutrition
October 30, 2021 8:52 am
As the COVID-19 pandemic is charting its course into 2022, as health care providers, we have had to adapt and adjust to the transient and shifting environment. Testing for COVID-19 has been in place, and is now part of the standard for preoperative work-up. In addition, covid testing will likely be part of screening any surgical procedure for the foreseeable future.
The challenge of pandemic control is the large pockets of populations in the US and worldwide that do not have protection against the virus and are not vaccinated. Vaccination provides the only proven long-term protection against COVID-19 infection and its long-term persistent health effect. In addition, the complication rate reported in scientific journals is negligible compared to the complication and death rate from the COVID-19 infection.
There are implications of covid infection and general anesthesia published in peer-reviewed journals. The increased risk of general anesthesia after covid infection is related to the severity of the initial infection and the extent of the treatment required, and the persistence of the post covid symptoms, including shortness of breath, fatigue, and laboratory finding elevated inflammatory markers. Long after resolution of the acute COVID-19 symptoms, the most common persistent complaints are fatigue, shortness of breath, Joint and chest pain; and all these increase the risk of post-operative complications (Carfì et al., 2020)
The required delay for surgery may be as short as 2-4 weeks to as long as six months or longer if the persistent symptoms are present. Surgery may not be avoidable in a critical life-threatening situation and may be necessary even with a much-increased risk of complication (Collaborative, 2020). Recovery post-COVID-19 may not be complete with the resolution of the initial symptoms (Dexter et al., 2020)
Recent publications and scientific presentations have also shown the protection that weight loss surgery and maintained weight loss provide in those who come down with the COVID-19 infection (Aminian et al., 2021). However, the rate of weight gain, lack of weight loss is worse for weight loss surgical patients post COVID-19 disorder (Bullard et al., 2021; Conceição et al., 2021). Furthermore, patients with COVID-19 infection post weight loss are at a higher risk of malnutrition (di Filippo et al., 2021; Kikutani et al., 2021). Up to 40% of patients have malnutrition if hospitalized with COVID (Anker et al., 2021).
To summarize, Weight loss and weight loss surgery reduce the severity of the initial COVID-19 infection. However, it increases malnutrition risk, requiring nutritional support and surgical interventions in non-responsive cases.
REFERENCES:
Aminian, A., Fathalizadeh, A., Tu, C., Butsch, W. S., Pantalone, K. M., Griebeler, M. L., Kashyap, S. R., Rosenthal, R. J., Burguera, B., & Nissen, S. E. (2021). Association of prior metabolic and bariatric surgery with severity of coronavirus disease 2019 (COVID-19) in patients with obesity. Surgery for Obesity and Related Diseases, 17(1). https://doi.org/10.1016/j.soard.2020.10.026
Bullard, T., Medcalf, A., Rethorst, C., & Foster, G. D. (2021). Impact of the COVID-19 pandemic on initial weight loss in a digital weight management program: A natural experiment. Obesity, 29(9). https://doi.org/10.1002/oby.23233
Conceição, E., de Lourdes, M., Ramalho, S., Félix, S., Pinto-Bastos, A., & Vaz, A. R. (2021). Eating behaviors and weight outcomes in bariatric surgery patients amidst COVID-19. Surgery for Obesity and Related Diseases, 17(6).
Di Filippo, L., De Lorenzo, R., D’Amico, M., Sofia, V., Roveri, L., Mele, R., Saibene, A., Rovere-Querini, P., & Conte, C. (2021). COVID-19 is associated with clinically significant weight loss and risk of malnutrition, independent of hospitalisation: A post-hoc analysis of a prospective cohort study. Clinical Nutrition, 40(4). https://doi.org/10.1016/j.clnu.2020.10.043
Kikutani, T., Ichikawa, Y., Kitazume, E., Mizukoshi, A., Tohara, T., Takahashi, N., Tamura, F., Matsutani, M., Onishi, J., & Makino, E. (2021). COVID-19 infection-related weight loss decreases eating/swallowing function in schizophrenic patients. Nutrients, 13(4). https://doi.org/10.3390/nu13041113
Sleeve Gastrectomy in Adolescent patients
September 23, 2020 5:44 am
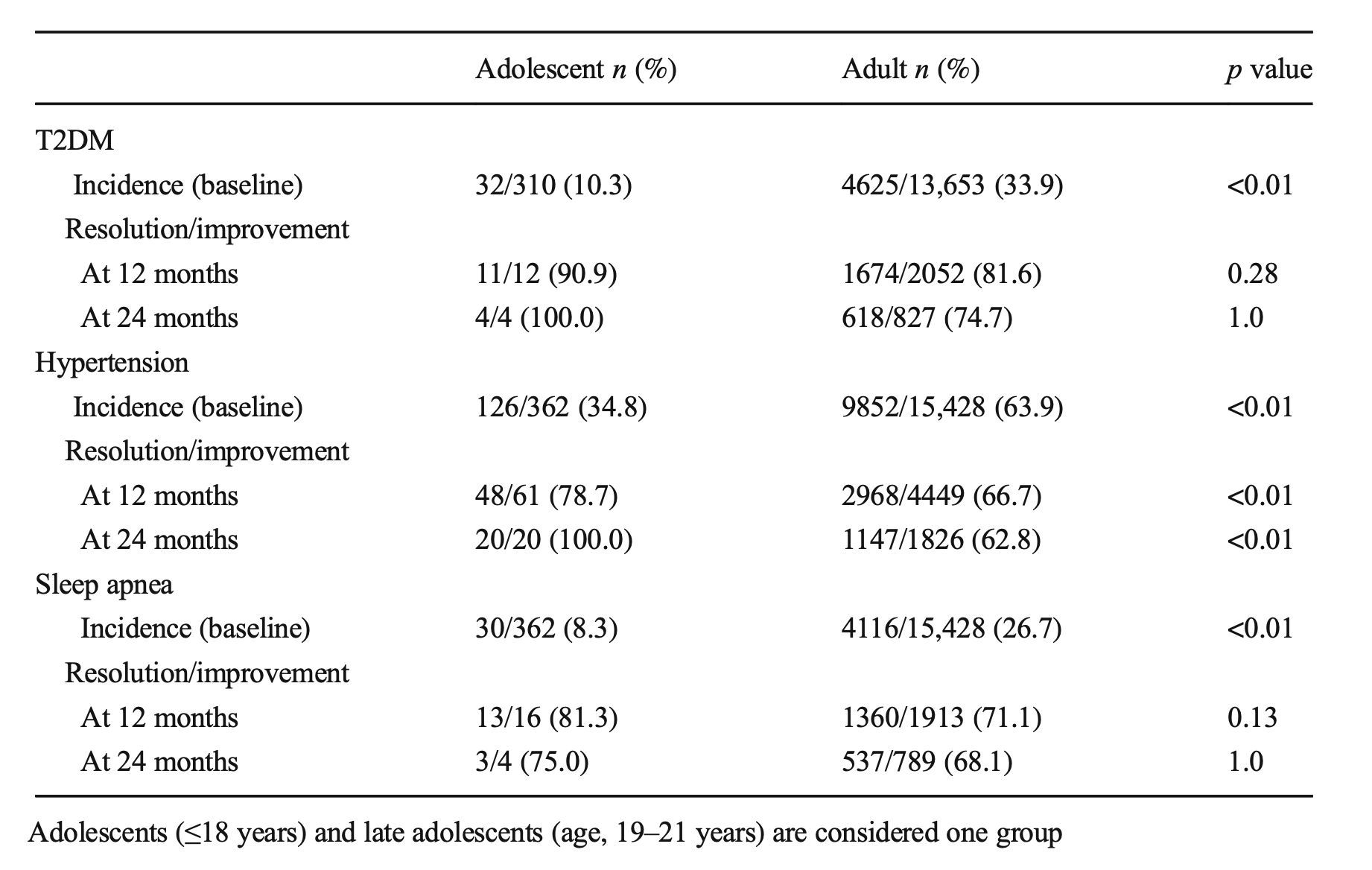 Sleep apnea resolved at the same rate. These early interventions can mean there may be lower long-term risk and associated conditions for these teens as they age.
A recent article was written from several adolescent weight loss surgical patients’ perspectives: This included their feelings of hope for their futures and health.
Sleep apnea resolved at the same rate. These early interventions can mean there may be lower long-term risk and associated conditions for these teens as they age.
A recent article was written from several adolescent weight loss surgical patients’ perspectives: This included their feelings of hope for their futures and health.
Zoom Group Meeting
September 21, 2020 7:10 am
We are excited to announce we will be having a Zoom group meeting Tuesday, September 22, 2020 at 7:00 PM PST. We hope to see you online!
Registration is required. Please follow the link to the meeting registration.
Vitamin D and Covid -19
May 07, 2020 9:24 am
We are all aware of the many roles that Vitamin D plays in our bodies. This includes immune function in addition to all the regulatory roles that Vitamin D plays in several physiologic reactions. There may be a correlation of low Vitamin D and COVID-19 infection increasing death risk as looked at in research articles.
Covid -19 in a subset of patience causes significant lung injury. These patients require mechanical ventilation.
Previously reported publications have suggested a possible correlation between ace inhibitors and increased risk of pulmonary complications of Covid -19. Some researchers suspect that the Covid-19 may be able to enter lung cells by the ACE receptors.
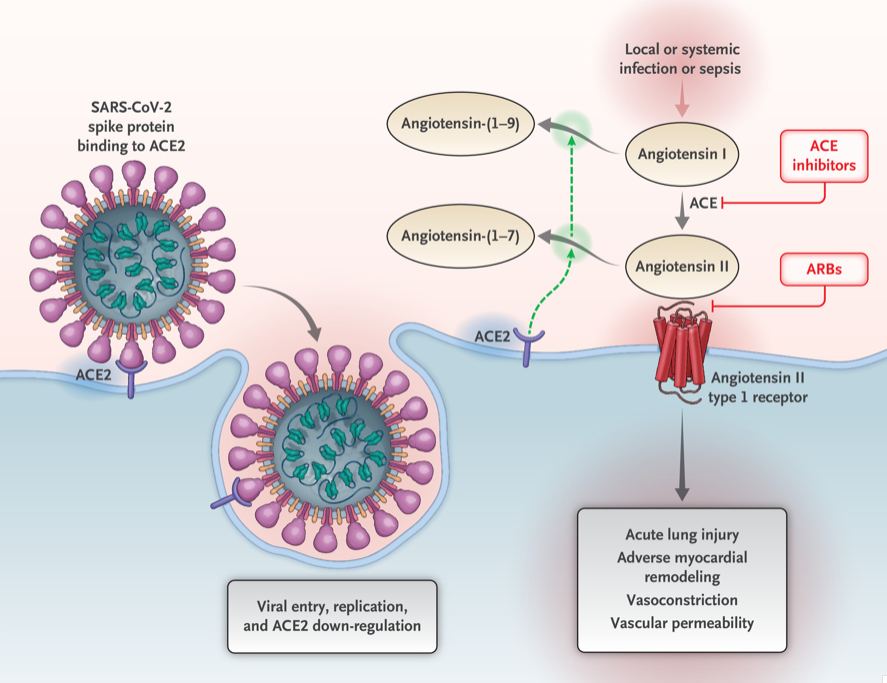
Vitamin D may positively implact the receptor ACE2. This study, report clear correlation between the high death rate with low vitamin D levels in Covid infected patients. There are limitation to this study that the attached abstract outlines.
Our take home message would be to please make sure you have updated labs and that you are all taking the recommended Vitamin D based on your surgical anatomy and laboratory values, not just an average non-bariatric person recommended dose.
https://www.dssurgery.com/wp-content/uploads/2020/05/manuscript.pdf
Copper Metabolims And Weight Loss Surgery
May 01, 2020 12:31 am
Written By: Osheen Abnous, Maria Vardapetyan, Eric Baghdasaryan
Copper is an essential element to all organisms, and it is a contributor in several enzymes vital to the function of hematopoietic, vascular, and skeletal tissues, as well as the structure and function of the nervous system.
As a crucial metal, copper plays an important role in chemical reactions throughout the human body; this includes the central nervous system. Enzymes are substances that facilitate chemical reactions. There are many copper-dependent reactions in the human body. In humans, the major site of absorption of dietary copper is still unclear. Copper in humans is absorbed in the proximal small bowel, duodenum, and ileum. This is after it has passed the acidic environment of the stomach.
Copper deficiency can be caused by malnutrition, prematurity, parenteral or enteral feeding without copper supplementation, gastrectomy, and excessive zinc therapy. The common causes of copper deficiency have been zinc supplementation, and changes to the PH (acidity) of the stomach. This can be the result of the alteration of the stomach anatomy, and by chronic acid suppression by proton pump inhibitors (antacids), and similar medications. Physicians need to be alert with patients who show signs of copper deficiency or are at a high risk of developing a copper deficiency.
It is important to raise greater awareness about copper deficiency because there is a growing number of patients undergoing surgeries for obesity, as the occurrence of copper deficiency will increase in the future.
Studies of patients who have had weight loss surgery in the past experience common symptoms such as pain involving the feet, gait abnormality (unusual walking), lower limb weakness, and recurrent falls. Common lab results include unusually low serum copper and serum ceruloplasmin levels. In some cases, elevated zinc levels are also present. Treatment includes cupric sulfate infusion until normal copper levels are reached, which then need to be maintained for the future. Vitamin B-12 deficiency has also been reported as a possible cause of myelopathy, which is a nervous system disorder that affects the spinal cord. As stated earlier, neurological damages are often irreversible and cause permanent damage to patients. Early diagnosis from physicians is crucial for patients who have undergone gastric bypass surgery, and the sooner they are diagnosed, the less permanent damage the patient will endure.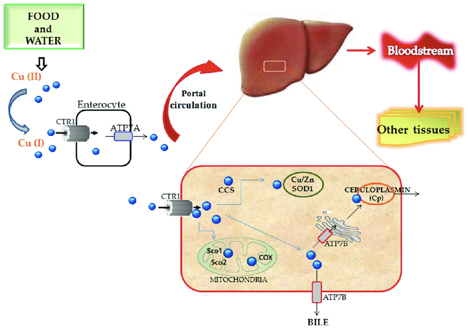
Case Discussions:
A 49-year-old woman had gastric bypass surgery for obesity 24 years age. She presetend with increasing lower limb stiffness and numbness. Additionally she reported tingling of the feet. As her pain continued to increase, she began using a walker, and her symptoms continued to worsen. After undergoing a neurological examination, results showed that the patient had increased lower limb tone and an absent perception of vibration at the toes and ankles. Laboratory results showed that the patient had copper levels barely detectable. This included serum copper and serum ceruloplasmin levels. In addition, the patient had reduced serum carotene (vitamin A) levels.
The patient received cupric sulfate intravenously daily through an 8-week period. After each daily infusion of cupric sulfate, the patient reported to have slight decreases in numbness and an increased tingling sensation. After the 8-week period, lab results showed that serum copper levels were normal and are needed to be maintained. Her night blindness was corrected by vitamin A injections.

In another case, a 53-year-old woman had symptoms of abnormal gait (abnormal walking) and anemia (lack of healthy red blood cells), and was seen for evaluation. The patient complained of pain in the lower legs, which would worsen over time and move up towards her thighs. As her ability to walk continued to worsen, the patient resorted to using a wheelchair. Her medical history consisted of an RYGB surgery for obesity. The only significant supplementation she received was 1000 μg vitamin B12 subcutaneously for several years. She had absent positional and vibratory sensation in the lower extremities to the knee. In addition, touch sensation was decreased. Laboratory examination revealed an elevated serum zinc level, and extremely low serum copper and ceruloplasmin levels.
For treatment, the patient received intravenous copper over a 6-day period, was discharged home, and then received weekly intravenous copper infusions thereafter. After a month of receiving intravenous copper, serum copper levels returned to normal. In addition, the patient’s pain in the lower leg improved, but vibratory sensation remained absent in the same area. Four months after being discharged from the hospital, the patient began walking with a cane.
Fat Soluble Vitamins
April 26, 2020 10:20 am
Written By: Maria Vardapetyan, Eric Baghdasaryan, Osheen Abnous
Vitamins are chemicals that facilitate many processes in the human body such as blood clot formation, good vision, fight infections etc. There are two classes of vitamins. Water soluble vitamins and fat soluble vitamins. Water soluble vitamins dissolve in water. This makes it possible for them to be absorbed through all mucous membranes. Fat soluble vitamins on the other hand do not dissolve or pass through mucous membranes. Fat-soluble vitamins are absorbed in the intestine along with fats in the diet. These vitamins have the ability to be stored in the fat tissues of the human body. Water-soluble vitamins are not stored in the body and have to be taken in daily with the food and dietary supplements. Solubility of a vitamin is not a function of its physical state. There are fat soluble vitamins that have a liquid form and almost all of the water soluble vitamins come in form of pills or powders.
In this article, we are going to focus on fat soluble vitamins. They are all complex molecules made of carbon, hydrogen, and oxygen in different arrangements (see figures 1, 2, 3 and 4). These fat soluble vitamins are vitamin A, D, E and K.
Vitamin A
Vitamin A has a major role in vision, immune function, cell growth, and maintenance of organs such as heart, kidneys, lungs, etc. It plays a pivotal role in the health of our eyes, specifically the retina1. Rhodopsin protein, a major protein that has the leading role in the process of vision, is found in the retina where it allows us to perceive light. This protein requires vitamin A to function properly. Without vitamin A, rhodopsin cannot sense light and thus cannot initiate the process by which vision occurs.

Figure 1: Chemical structure of Vitamin A molecule
Vitamin D
Vitamin D regulates different chemical reactions that are associated with bones, muscles, and the immune system. The simplified way it does this regulation is it helps absorb calcium from dietary nutrients which in turn strengthens the bones, helps neurons exchange signals to move muscles and helps the immune system to fight against viruses and bacteria2.
 Figure 2: Chemical structure of Vitamin D molecule
Figure 2: Chemical structure of Vitamin D molecule
Vitamin E
Vitamin E acts as an antioxidant. Antioxidants are naturally occurring chemicals that neutralize toxic byproducts of many chemical reactions in the human body. When food is consumed and digested, the human body converts it into energy. As a result of metabolism free radicals (toxic byproducts) are formed and are neutralized with the help of vitamin E. In addition, free radicals are also in the environment. Furthermore, vitamin E stimulates the immune system to fight against bacteria and viruses3.
 Figure 3: Chemical structure of Vitamin E molecule
Figure 3: Chemical structure of Vitamin E molecule
Vitamin K
Vitamin K can be obtained from food and dietary supplements. There are two forms of vitamin K: phylloquinone (Vitamin K1), which is found in spinach, kale and other greens and menaquinone-4 (Vitamin K2), which is found in animal products. Vitamin K1 is involved in blood clotting, and Vitamin K2 is involved in bone tissue building. Vitamin K1 is the main Vitamin K in human diet (75-90% of all vitamin K consumed), however, it is poorly absorbed in the body4,5.

Figure 4: Chemical structures of Vitamin K1 and K2 molecules
Absorption of fat soluble vitamins
Polarity describes the inherent charge(positive or negative) or lack of charge for any given substance or molecule. Molecules that are charged are referred to as “polar”, while those that lack charge are “nonpolar”. When discussing solubility, it is important to remember the phrase “like dissolves like”. That means polar (charged) substances like to interact with a polar environment like water, since water contains a slight negative charge. Hence, charged substances are water-soluble. Nonpolar substances on the other hand readily interact with nonpolar environments such as fat, which contains no charge. Therefore, molecules that lack a charge such as vitamins A, D, E, and K are referred to as fat soluble.
Due to their water fearing nature, these fat soluble vitamins cannot simply be absorbed directly into the bloodstream (which is mostly water) like the sugars and amino acids in our diet. As their name suggests, these fat soluble vitamins like to be embedded in fatty droplets, which facilitate their absorption in the following way. Fat soluble vitamins group together with other fat molecules to form fatty droplets, effectively reducing the amount of interaction with the watery environment of the intestines. Therefore, without an adequate amount of fat in your diet, your body is unable to effectively absorb these fat-soluble vitamins. This may be true in an intact anatomy, however, post weight loss surgical patients can not increase their fat soluble vitamin levels by increasing their fat intake. This is due to the fact that a high fat diet causes excessive bowel movement which in turn washes away any vitamins taken by mouth. DS limits fat absorption (thus the great weight loss) which can cause vitamin A and D deficiency that can not be easily corrected with oral supplementation.
As mentioned before, fat soluble vitamins are hydrophobic and nonpolar, which means they are also fat loving or lipophilic. Excess fat soluble vitamins can be stored in the liver and fat tissue. Therefore, these vitamins do not need to be eaten every single day since stores of these vitamins can sustain a person for some time. It may take several weeks or months for our body to deplete these stores of fat soluble vitamins which is why it generally takes a longer amount of time for fat soluble vitamin deficiencies to manifest themselves. The ability to store these fat soluble vitamins in tissues can also lead to vitamin toxicity – marked by an excess of vitamin stores in our body.
Clinical manifestations of A, D, E, K deficiency
| Vitamin | Clinical Deficiency manifestations |
| Vitamin A | Vision Problems
Dryness of the eye |
| Vitamin D | Softening and weakening of the bones
Bone shape distortion Bowed legs (generally in children) Hypocalcemia |
| Vitamin E | Damage to red blood cells
Tissue/organ damage due to inability to supply enough blood Vision problems Nervous tissue malfunction |
| Vitamin K1 | Excessive bruising
Increased bleeding time Small blood clots under nails Increased bleeding in mucous membrane |
| Vitamin K2 | Weak bones
Increased plaque deposits along gumline Arterial calcification |
References
- Office of Dietary Supplements – Vitamin A. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/#. Accessed April 26, 2020.
- Office of Dietary Supplements – Vitamin D. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminD-Consumer/. Accessed April 26, 2020.
- Office of Dietary Supplements – Vitamin E. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminE-Consumer/. Accessed April 26, 2020.
- Vitamin K. The Nutrition Source. https://www.hsph.harvard.edu/nutritionsource/vitamin-k/. Published July 2, 2019. Accessed April 26, 2020.
- Beulens JWJ, Booth SL, van den Heuvel EGHM, Stoecklin E, Baka A, Vermeer C. The role of menaquinones (vitamin K₂) in human health. The British journal of nutrition. https://www.ncbi.nlm.nih.gov/pubmed/23590754. Published October 2013. Accessed April 26, 2020.
Biofilm
April 26, 2020 9:44 am
Written By: Eric Baghdasaryan, Maria Vardapetyan, Osheen Abnous
Biofilm are tiny microorganism-filled communities found throughout the human gastrointestinal tract and oral cavity. These communities adhere to both biological and non-biological surfaces within the human body. They provide their inhabitants with many competitive advantages that help these bacterial communities withstand biological, chemical, and physical stresses1. Within these communities, microorganisms collaborate with one another to increase the likelihood of growth and multiplication despite the harsh conditions of the human gut. Not all bacteria within these biofilms are harmful, but those that are go on to cause infections and other severe health problems for the host.
Biofilm formation
Studies have shown that approximately 60-80% of bacterial infections in the human body are associated with biofilm formation. Such findings have compelled researchers to investigate the complex factors responsible for biofilm formation.

Figure 1: Biofilm adhesion, formation, and maturation. whiteley.com.au/biofilms
It was shown that bacteria anchor themselves to the mocosa surface. They collectively form a protective layer made of polysaccharides, proteins, and extracellular DNA. This forms the biofilm matrix. This biofilm matrix acts as a shield against antimicrobials, toxins, and antibodies. From here, biofilm associated bacteria go on to cause chronic infections characterized by persistent inflammation and tissue damage, initiating in the gut and adjacent regions of the gastrointestinal tract. Furthermore, some biofilm associated bacteria have shown the ability to disperse from this mature biofilm to colonize new niches, underscoring the association between local infections and systemic diseases such as atherosclerosis and rheumatoid arthritis2 caused by the buildup of biofilm dispersed bacteria and subsequent inflammation in the coronary vasculature and joint capsules, respectively. In fact, BADAS syndrome (bowel associated dermatosis-arthritis syndrome) is a condition where patients present themselves with small bumps on their inner skin (mainly along the vasculature) caused by the buildup of circulating microtoxins (very small clusters of bacteria). This may lead to chronic bacteremia in the bloodstream. Also, the over circulation of host immune complexes presents many problems for the patients, such as the development of arthritis and the accompanying joint pain, caused by the build up of white blood cells in host joint capsules. Patients often link the lumps to a dermatological condition, when in reality the condition is caused by a bacterial overgrowth originating in the gut and bowel. Clinicians now believe it is very likely these bacteria are biofilm-associated and a proper early diagnosis of the biofilm origin is critical to the prevention of BADAS and similar pathologies3.
The formation of biofilms has been studied on foreign substances such as intravenous catheters, orthopedic implants, and other biomaterials that have shown device-associated infections. However, it is commonly accepted that the majority of chronic bacterial infections involve biofilm formation on natural surfaces. The pathogenic bacterial overgrowth, forming the biofilms, have been linked to major diseases of the gastrointestinal tract including Inflammatory bowel disease and colo-rectal cancer4.
In addition to the gastrointestinal tract, biofilms can also be formed in the oral cavity. Over 700 bacterial species reside in the oral cavity. These contribute to the outgrowth of oral biofilms (otherwise known as dental plaque, see figure 2). These oral biofilms are responsible for major oral diseases such as tooth decay, gingivitis, and periodontitis. Moreover, those with periodontal infections have significantly increased risk of cardiovascular diseases, including atherosclerosis, myocardial infarction, and stroke2. The inflammation caused by oral biofilm may also be a contributing cause of conditions such as diabetes and rheumatoid arthritis1. Therefore, the control of oral biofilm growth before the development of oral infections is critical for the prevention of these system conditions.

Figure 2: Oral Biofilm Formation.
https://phys.org/news/2018-10-scientists-infection-causing-biofilms.html
This symbiotic (mutually beneficial) relationship between gut microbiota (bacteria living in our gut) and the host begins at birth and is crucial to our overall fitness and health. However, certain external and internal factors modify the gut microbiota. This causes the formation of a pathogenic biofilm, which leads to detrimental health conditions. The same bacteria that was once helping us by maintaining a healthy gastrointestinal tract, is now triggering disease conditions4.
Due to bacteria’s ability to translocate, migrate, and colonize new surfaces or niches, biofilm associated infections in the gut have been linked to systemic infections in other organs, including the joints, the skin, the eyes, the vasculature, the lungs, and even the central nervous system. It is assumed that the formation of a thick mucosal biofilm might be used as a diagnostic biomarker for the onset of systemic diseases. The outgrowth of a biofilm is widely viewed as the tipping point between two alternative states: a healthy and diseased gut1.
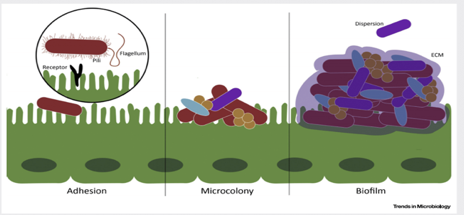
Figure 3. Biofilm matrix – a protective layer. Trends in Microbiology.
The biggest clinical challenge with biofilm-associated infections is their high resistance to antibiotic therapy. The effective therapeutic concentration of certain antibiotics to fight off bacteria within a biofilm (amount of the antibiotics needed in order to have positive therapeutic effects) is about 100-1000-fold higher than if the same bacteria were not associated with a biofilm2. The extracellular matrix, scaffold that keeps the bacteria anchored in place, prevents the penetration of host immune cells into the biofilm, thus contributing to the increased survival of the bacterial species living within the biofilm. Bacteria living within a biofilm also undergo an increased number of mutations, leading to the generation of more antibiotic-resistant phenotypes of bacteria. Finally, studies have shown that minimal concentrations of antibiotics may actually facilitate and stimulate biofilm formation, which can be extremely problematic in clinical treatment2. Therefore, to decrease the risk of biofilm induction, physicians should begin with very high doses of chemotherapeutics (antibiotics) from the very beginning of diagnosed infection. Looking ahead, there is clearly a need for novel biofilm-targeted therapies that are specifically made to prevent biofilm formation as well as eliminate the biofilm completely once it has already matured. Researchers have identified several drug candidates – DNase, lactoferrin, chlorhexidine, and taurolidine2 – that they believe have the potential to effectively penetrate and destroy components of the biofilm matrix. Further research is needed to determine their efficacy.
References
- Tytgat HLP, Nobrega FL, van der Oost J, de Vos WM. Bowel Biofilms: Tipping Points between a Healthy and Compromised Gut? Trends in Microbiology. January 2019;27(1): 17-25. doi:10.1016/j.tim.2018.08.009.
- Marcinkiewicz J, Strus M, Pasich E. Antibiotic Resistance: a “dark side” of biofilm-associated chronic infections. Polskie Archiwum Medycyny Wewnetrznej (Polish Archive of Internal Medicine). 2013;123(6):309-312.
- Buret AG, Motta JP, Allain T, Ferraz J, Wallace JL. Pathobiont release from dysbiotic gut microbiota biofilms in intestinal inflammatory diseases: a role for iron? Journal of Biomedical Science. January 2019;26(1) doi:10.1186/s12929-018-0495-4
Diabetes and Weight Loss Surgery
April 06, 2020 5:51 am
The scientific literature is riddled with evidence pointing to the benefit of early metabolic surgery as a superior treatment, remission and possible cure option for diabetes. Unfortunately, the medical education, pharmaceutical companies, primary care healthcare delivery systems and third party payers (health insurance companies) have not caught up with the published data. The American Diabetes Association has changed their guidelines to reflected the benefit for combating diabetes with weight loss surgery.
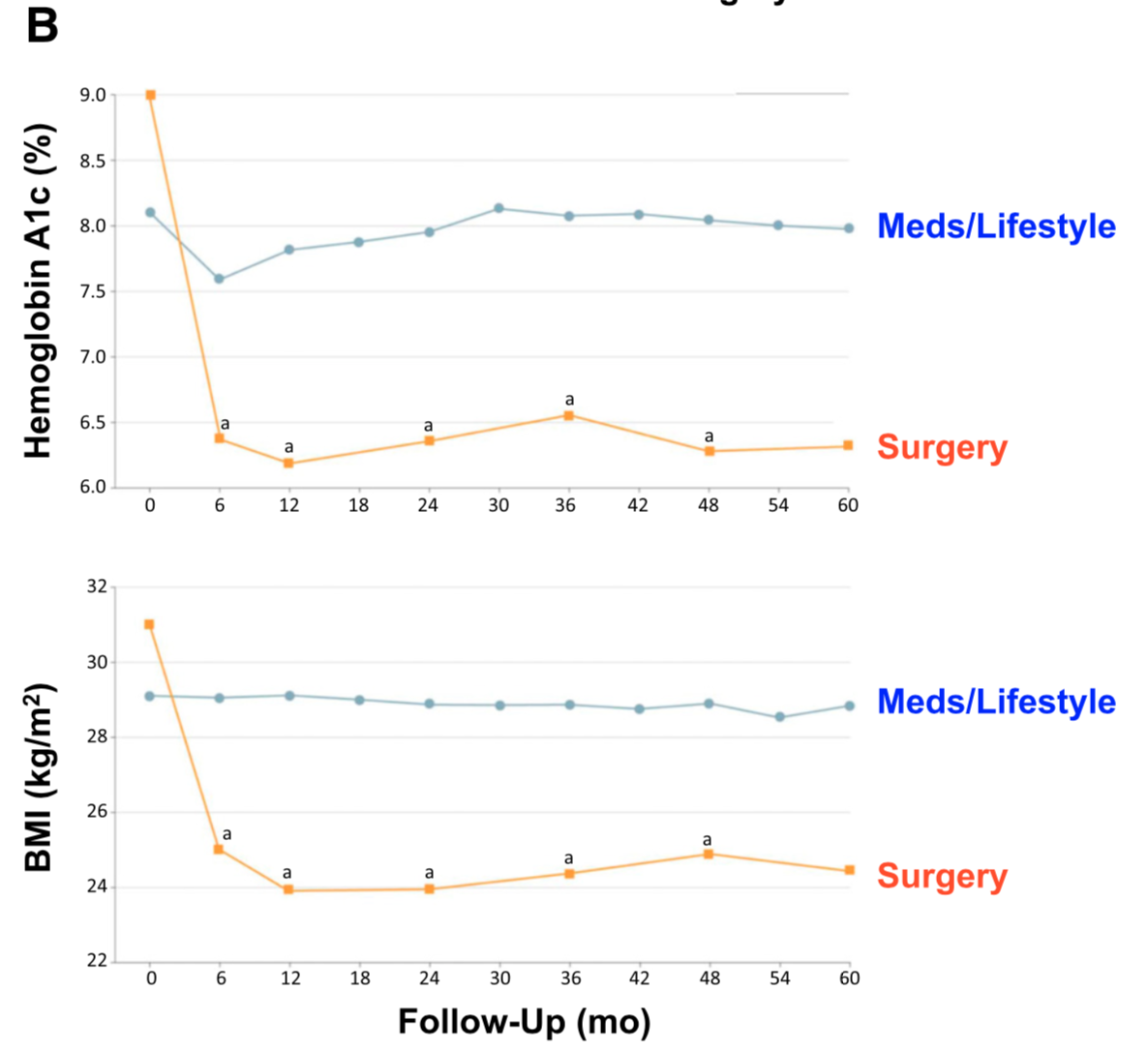
There is ample evidence of the superior outcome of surgery as a treatment option for diabetes when compared to medical managment. Cummings et.al, in a published article in Diabetes Care, showed sustained stabilization of the Hemoglobin A1C six years after surgery. In contrast, there was no significant changes noted in the non-surgical group.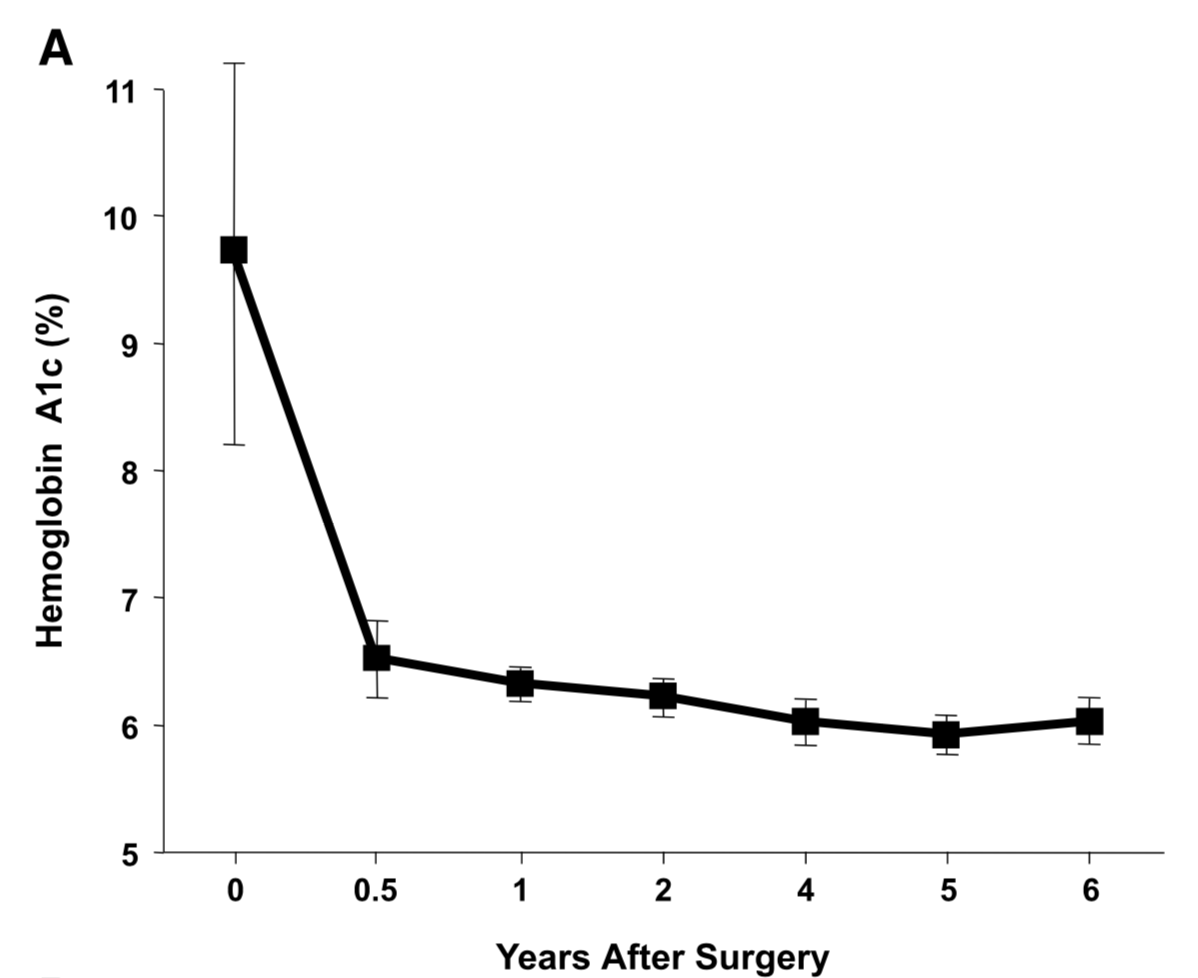
Jans et.al. , in November of 2019 showed that the patients who had NOT been on Insulin, and had metabolic surgery had the highest long term success for resolution and remission of the diabetes. This identifies that having a patient be proactive in their care by having metabolic surgery improves success rates.
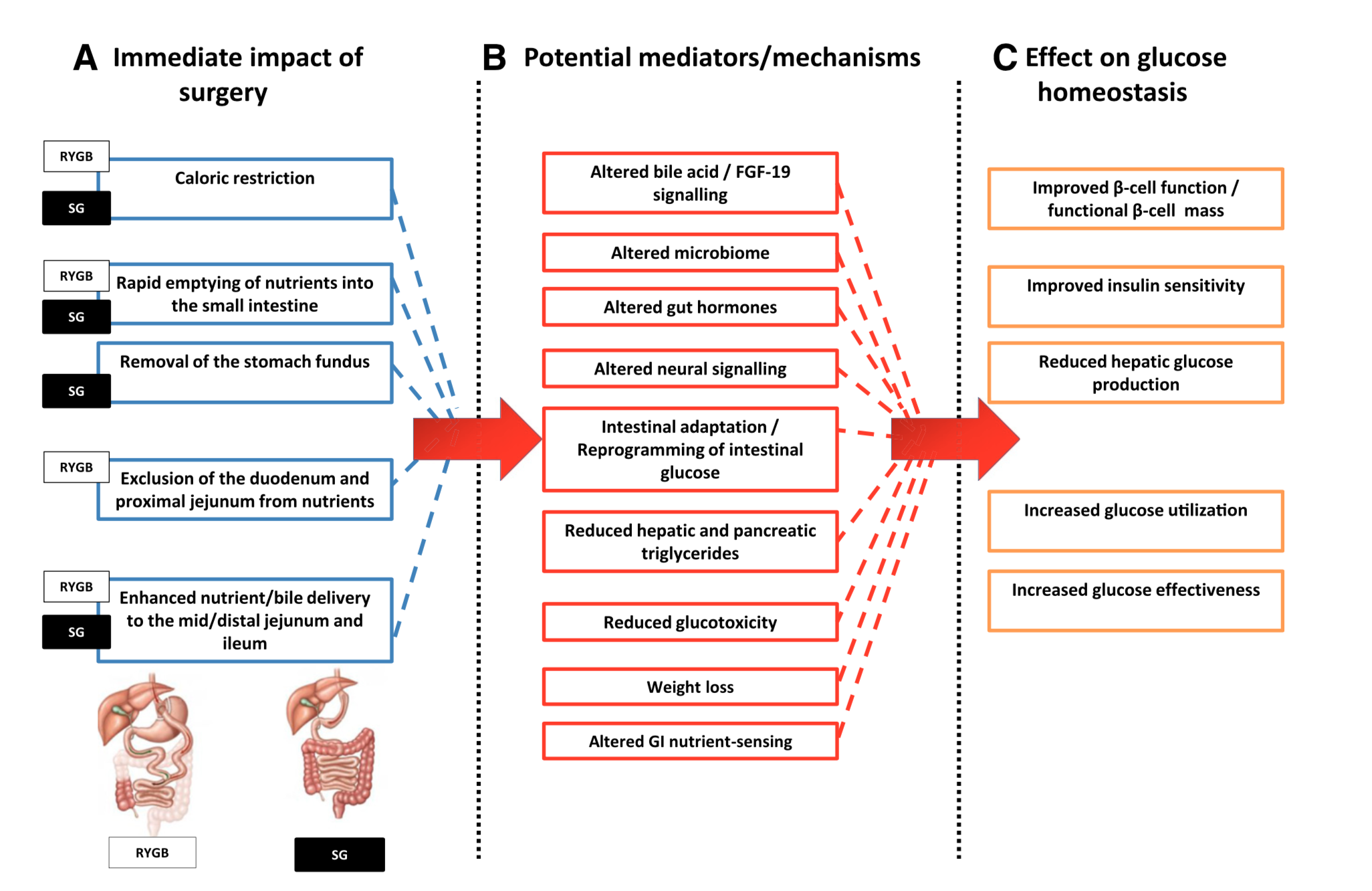
The exact mechanism by which the diabetes is resolved is unclear. The weight loss may play a role. There are numerous hormones and neuroendocrine modulators which control the complex metabolic pathways. Batterham et.al., in Diabetes Care (2016), published a summary overview of the possible mechanism involved in diabetes improvement following metabolic surgery.

There are a number of overlapping and sequential layers for possible reasons why diabetes resolves after weight loss/metabolic surgery. These may be directly related to surgery and the reduction of the calorie intake or absorption. It may also involve the neuroendocrine modulators.
What can be said definitively is that early surgical intervention is best and most likely the only permanent solution to type II diabetic resolution. There is no medical justification in not considering metabolic surgery in diabetic patients who may also have difficulty with meaning a BMI< 35.