
July 2, 2014 Group Meeting Recap
July 03, 2014 7:11 am
First and foremost, We apologize for the confusion and last minute change with the webinar. It was set to go and logged in then the internet dropped the group meeting. The meeting site automatically marked the meeting as over. We sent out e-mails with the new URL for the group meeting but it took time. Thank you for your patience with this new platform. Although far reaching, it comes with downsides and hopefully we can make this a long term way to reach our patients. Lesson learned, don’t rely on wireless internet access for webinars. The Anemia slides will be added to our website dssurgery.com soon.
Ferritin is a protein that acts like your savings account. It’s like a holding tank. When you have a blood loss your body goes to Ferritin stores for iron to increase red blood cell production. Iron is like money in your pocket. For small and daily building of red blood cells. Transferrin is a protein transport that carries the iron. Copper is also needed to transport iron. Iron can be readily available but will not be utilized unless your protein levels are adequate. The protein level on laboratory studies needs to be at least 6 gm/dL & Albumin 3.2 gm/dL for adequate iron utilization. Vitamin B12 also is needed for iron utilization.
Iron metabolism in the DS patient is limited due to several factors. In unaltered anatomy Iron enters the stomach where it is exposed to acid and changes into a form which allows it to be absorbed. Then it enters the duodenum which is the chief area of the small intestines where iron absorption takes place. There is possibly a second minor site of absorption near the end of the ileum. However, after the DS there is a small portion of the duodenum that is left after the pyloric value for iron absorption. Below is a list of iron rich foods. Also remember to take Vitamin C with your iron supplements and when eating plant based iron rich foods add a food that is high in Vitamin C.
There was a brief discussion regarding Calcium oxalate kidney stones. That talk can be found on our website. Treatment is limiting oxalate containing foods and to increase calcium supplements to 3,000mg daily but to take half with food and the other half without food. Also Vitamin K2 can also decrease kidney stones.
Fissures where also briefly discussed. Fissures are most likely caused by the unopposed bile salts entering the colon after DS. Bile is alkaline and causes irritation to the mucosa. Treatment is liberal use of barrier type creams/ointments, controlling loose stools by watching if certain food items cause them or by using fiber with half the liquid mixed with it. The fiber with less liquid acts as a sponge to give more form to the stool.
We had anemia themed snacks at the live group meeting. Pate, Southwest ground Bison, and a Mayan Pumpkin seed dip. Here is the information on the nutritional value of Bison versus other meats. It is higher in iron and Vitamin B12 and lower in fat and cholesterol.
Iron Content of Common Foods
This chart shows the amount of total iron in food. Iron from most animal sources (heme iron) usually is more readily absorbed than iron from plant sources of food (non-heme iron). Include a source of vitamin C or heme iron to improve the absorption of non-heme iron.
Sources of Predominantly Heme Iron
|
FOOD
|
IRON (MILLIGRAMS)
|
|
Beef liver, braised (3 oz)
|
5.8
|
|
Lean sirloin, broiled (3 oz)
|
2.9
|
|
Lean ground beef, broiled (3 oz)
|
1.8
|
|
Skinless chicken breast, roasted dark meat (3 oz)
|
1.1
|
|
Skinless chicken breast, roasted white meat (3 oz)
|
0.9
|
|
Pork, lean, roasted (3 oz)
|
0.9
|
|
Salmon, canned with bone (3 oz)
|
0.7
|
Sources of Non-Heme Iron
|
FOOD
|
IRON (MILLIGRAMS)
|
|
Fortified breakfast cereal (1 cup)*
|
4.5 – 18
|
|
Pumpkin seeds (1 oz)
|
4.2
|
|
Blackstrap molasses (1 Tablespoon)
|
3.5
|
|
Soybean nuts (1/2 cup)
|
3.5
|
|
Bran (1/2 cup)
|
3.0
|
|
Spinach, boiled (1/2 cup)
|
3.2
|
|
Red kidney beans, cooked (1/2 cup)
|
2.6
|
|
Prune juice (3/4 cup)
|
2.3
|
|
Lima beans, cooked (1/2 cup)
|
2.2
|
|
Tofu, firm (1/2 cup)
|
2.0
|
|
Enriched rice, cooked (1/2 cup)
|
1.4
|
|
Pretzels (1 oz)
|
1.2
|
|
Whole-wheat bread (1 slice)
|
0.9
|
|
Green beans, cooked (1/2 cup)
|
0.8
|
|
White bread, made with enriched flour (1 slice)
|
0.8
|
|
Egg yolk, large (1)
|
0.6
|
|
Peanut butter, chunky (2 tablespoons)
|
0.6
|
|
Apricots, dried (3)
|
0.6
|
|
Zucchini, cooked (1/2 cup)
|
0.3
|
|
Cranberry juice (3/4 cup)
|
0.3
|
|
Unenriched rice, cooked (1/2 cup)
|
0.2
|
|
Grapes (1/3 cup)
|
0.1
|
|
Egg white, large (1)
|
From: The American Dietetic Association’s COMPLETE FOOD & NUTRITION GUIDE, 2nd ed. 2002.
USDA National Nutrient Database
Diabetes and Weight loss Surgery
June 30, 2014 5:44 pm
Diabetes should be considered as a family of diseases sharing a common name. They are different diseases because the cause, pathophysiology, and the treatment options are different for each diseases. This is not to say that there are not commonalities between them.
- Type I (Insulin deficiency, Juvenile onset)
- Type II (Insulin Resistance, Adult onset)
- Latent Autoimmune diabetes (LADA)
- Gestational
Type I diabetic patients requires insulin for control of their blood sugar. Insulin deficiency is the underlying problem with type I diabetes. The causes of type I diabetes are many and some are poorly understood. It is presumed that viral infections, genetics, infections, chronic pancreatitis and autoimmune conditions may all be potential causes of type I diabetes.
Type II diabetes is an insulin resistance state. This means that the patients’ body may be making adequate level of insulin however, for a number of reasons, the insulin is not able to normalize the blood sugars. Some Type II diabetic patients may also require insulin during advanced stages, but in most cases the initial treatment is oral medications.
| Diabetes Type | Blood Sugar | Blood Insulin |
| Type I | High | Low-absent |
| Type II | High | High(early disease state) |
The table above summarizes the laboratory findings in a patient who is diagnosed with diabetes. The measured insulin can be distinguished in the labs as being injected or patients own.
LADA is probably a subtype of Type I, with a delayed presentation. It behaves like Type I, with insulin deficiency, yet it is adult onset.
Gestational is more of a high blood glucose state during the pregnancy.
The goal of medical treatment for diabetes has been to normalize the blood sugars. There are no medical treatments regimens that correct any of the underlying causes of the Type I, or Type II.
In the case of Type I, the underlying case is Insulin deficiency. The definitive treatments may include Pancreatic transplantation, and intelligent Insulin pumps.
Surgical treatment of Type II, by some know and unknown mechanisms, corrects the underlying resistance to the insulin.
Weight loss surgical procedures have been shown to “cure” Type II”. The “remission” or “cure” rate of diabetes is really different between surgical procedures. Duodenal switch operation has been shown to have the highest remission-cure rate of all surgical procedures for the Type II diabetes. The references are available on our website. By definition, Type I can not be corrected-cured with weight loss surgery, since the underlying problem is insulin deficiency. What we have experienced however is that the Insulin requirements significantly decreases and blood glucose control is much easier after weight loss surgery.
There have been a number of articles reporting high relapse rate of Type II in gastric bypass patients. This is why I have always advocated that the patients with metabolic conditions, including diabetes should only consider the duodenal switch as their only surgical option.
The one study of 4434 patients, 68.2% of those patients who had Type II had remission within 5 years after the gastric bypass procedure. 35% of those patients, however, had a redevelopment of Type II after 5 years. “When the patients that never remitted and those that relapsed were added together, more than half of the patients (56%) did not have durable remission of diabetes.” (Obes Surg 2012 Nov 18:doi 10.1007/s11695-012-0802-1).
An article published in May 2010, reported 24% recurrence or worsening of the diabetes in patients who have had gastric bypass operation. (SOARD Volume 6, issue 3, May 201 249-253).
Single-Anastomosis DuodenoIleal Bypass (SADI)
June 23, 2014 6:30 pm
Single anastomosis duodenal switch, also known as Single Anastomosis DuodenoIleal Bypass (SADI) is a procedure that is being discussed in literature. There have been a few series of case reports that have been published in the last few years. I would like to review the procedure and share my opinion.
The theory behind the SADI has been to simplify the duodenal switch procedure. In “classical” duodenal switch procedure, the small bowel is divided in two places, (duodenum, and distal ileum) and two anastomosis are created (duodeno-ileostomy, and ileo-lieostomy). This can theoretically provide two potential places for leak, bleeding, adhesions as complications. In SADI, there is a single bowel division of the duodenum and a single anastimosis of the duodenum and the ileum. The sleeve component of the procedure is the same for both procedures. This is where their similarities end.
In the duodenal switch operation, the bowel is partitioned in to two parallel limbs- one that carries the biliopancreatic juices and a parallel limb that bring the food down from the post pyloric duodenum. They then join and form the common channel. The length of the biliopancreatic limb is so long that it does not allow bile to reflux back into the duodenum or back to the stomach causing the complication of bile reflux gastritis. With the single anastomosis of the SADI, the length of the bowel where the bile meets the duodenum is shorter than it is in normal anatomy. This significantly increases the possibility of the bile reflux. The second difference is the selective nature of the reduced absorption of the fat in the duodenal switch, in comparison to that of the carbohydrates. Duodenal switch operation has two absorptive lengths- the Alimentary channel, which is involved with protein and carbohydrate absorption, and the common channel that absorbs, fat, protein and carbohydrates. One can make changes to the common channel and impact the fat absorption significantly more than that of the carbohydrate and the proteins. In SADI procedure, that common channel and the alimentary limb are both the same- there is no way to selectively adjust the fat absorption without making significant changes to that of the protein and carbohydrate absorption.
There are a number of publications that have reported the short-term outcome of the SADI procedure. They appear promising, but they are short-term results. Long-term data is needed. If the outcome does not change significantly over time, then I could see a role for SADI in the treatment for obesity. In the mean time, patients need to be made aware that the suggestion that SADI is the same as the duodenal switch is probably not correct since we do not have the data to support this oversimplification.
Single-Anastomosis DuodenoIleal Bypass (SADI), SIPS, Loop
June 23, 2014 1:45 pm
Single anastomosis duodenal switch, also known as Single Anastomosis DuodenoIleal Bypass (SADI) is a procedure that is being discussed more frequently in the literature. There have been a few series of case reports that have been published in the last few years. I would like to review the procedure and share my opinion.
The theory behind the SADI has been to simplify the duodenal switch procedure. In “classical” duodenal switch procedure, the small bowel is divided in two places, (duodenum, and distal ileum) and two anastomosis are created (duodeno-ileostomy, and ileo-lieostomy). This can theoretically provide two potential places for leak, bleeding, adhesions as complications. In SADI, there is a single bowel division of the duodenum and a single anastomosis of the duodenum and the ileum. The sleeve component of the procedure is the same for both procedures. This is where their similarities end.
In the duodenal switch operation, the bowel is partitioned in to two parallel limbs- one that carries the biliopancreatic juices and a parallel limb that bring the food down from the post pyloric duodenum. They then join and form the common channel. The length of the biliopancreatic limb is so long that it does not allow bile to reflux back into the duodenum or back to the stomach causing the complication of bile reflux gastritis. With the single anastomosis of the SADI, the length of the bowel where the bile meets the duodenum is shorter than it is in normal anatomy. This significantly increases the possibility of the bile reflux. The second difference is the selective nature of the reduced absorption of the fat in the duodenal switch, in comparison to that of the carbohydrates. Duodenal switch operation has two absorptive lengths- the Alimentary channel, which is involved with protein and carbohydrate absorption, and the common channel that absorbs, fat, protein and carbohydrates. One can make changes to the common channel and impact the fat absorption significantly more than that of the carbohydrate and the proteins. In SADI procedure, that common channel and the alimentary limb are both the same- there is no way to selectively adjust the fat absorption without making significant changes to that of the protein and carbohydrate absorption.
Other than the obvious anatomical variations described above, it is important to mention that the concerns outlined above are mostly theoretical.
There are a number of publications that have reported the short-term outcome of the SADI procedure. They appear promising, but they are short-term results. Long-term data is needed. If the outcome does not change significantly over time, then I could see a role for SADI in the treatment for obesity. In the mean time, patients need to be made aware that the suggestion that SADI is the same as the duodenal switch is probably not correct since we do not have the data to support this oversimplification.
The animation of the Duodenal switch is here.
For comparison of duodenal Switch and SADI please check our web site here.
Phytates the anti-nutrient?
June 20, 2014 3:33 pm
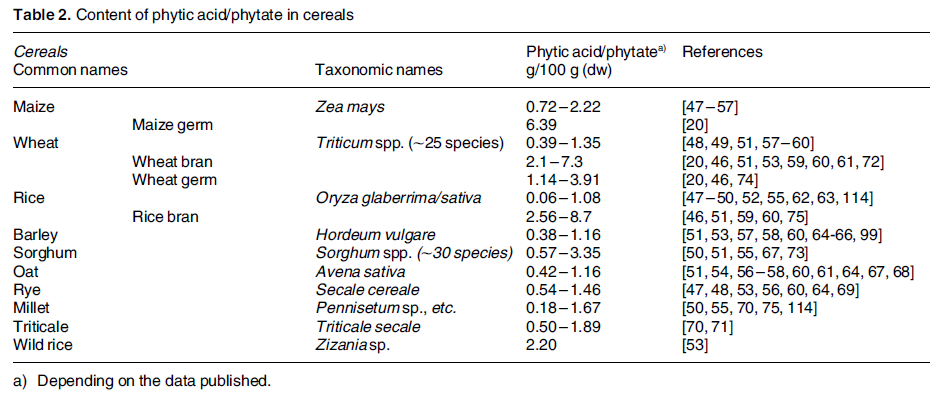
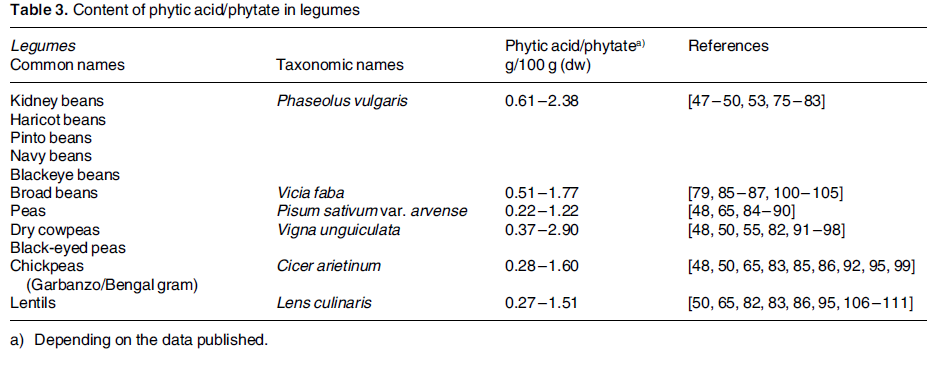
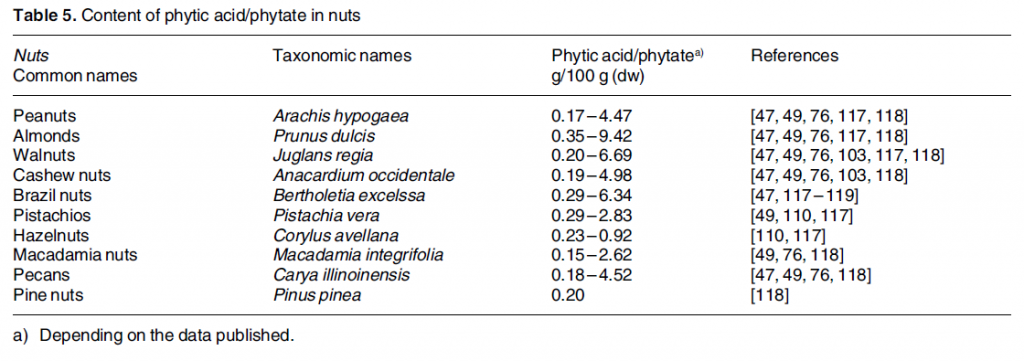
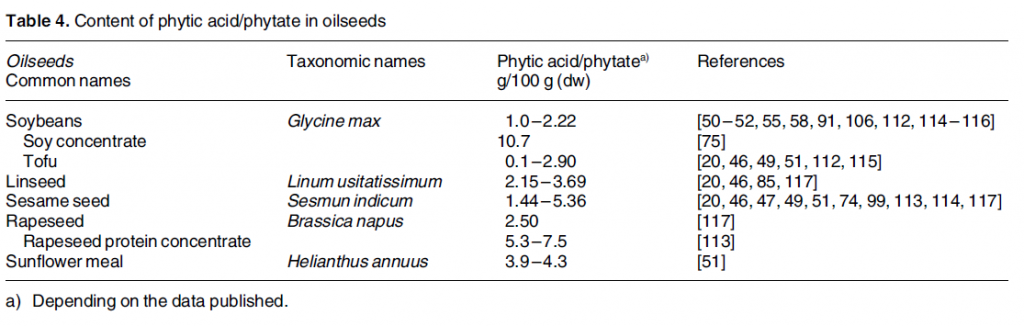
Phytic acid is phosphorus stores in nuts, edible seeds, beans/legumes, and grains. It is often referred to as anti-nutrient. Phytates (phytic acid) have been shown to decrease absorption of minerals, including iron, calcium, zinc and manganese. Phytates decrease the absorption by binding to the minerals before their uptake in the stomach and intestines. 5-10mg of phytic acid can decrease iron absorption by 50%. 1 This research done on non-WLS patients but is something to be aware of if you are having iron deficiency anemia or low calcium issues.
There are ways to combat the effects of phytic acid such as heat, soaking, fermenting, Vitamin C, protein, probiotics, and sprouting. 2
Phytic acid has many benefits such as preventing kidney stones, anti cancer effects, cardiovascular health protectant, binding with heavy metals and free radicals. It becomes an antioxidant and is a secondary messenger in cellular activity.
Phytate intake is something to be looked at if you are experiencing iron or calcium deficiencies.Adjusting your intake of phytates containing foods, combining them with high Vitamin C containing food items, and/or prepping them before consumption can decrease the mineral binding capacity. It would also be prudent to be aware of the timing between eating phytic acid containing foods and any vitamin or mineral supplementation.
Shared Success Story: Cyndi E. Had a Gastric Bypass to Duodenal Switch Revision
June 17, 2014 6:29 am
My journey to lose weight has taken most of my life. Losing weight is not just about food or eating too much, but a combination of genetics, emotions, and habits. My experience began at age 13 and has continued throughout my life. I have tried everything! I had a previous RNY Gastric Bypass, and knew something was wrong. I had seen another Bariatric surgeon who said there is nothing I can do for you because you failed. My primary Doctor asked me “does your husband love you?” Of course, but what does that have to do with me knowing there is something medically wrong with me? Again, I was brushed off and told to come back in two weeks. Leaving that day, I knew I was never going back. I went home and googled, “Bariatric Surgeon”, as I had for the past 3-4 years. Then, through a series of events was put in touch with Barbara Metcalf, a bariatric nurse, who lived in my town. As I explained my story to Barbara, she shared information with me about Duodenal Switch operation, and gave me names of two surgeons.

I contacted Dr. Ara Keshishian, in Glendale, and had a consultation that week. Meeting “Dr. K” was amazing! It was the first time a Doctor did not blame me for my weight. He explained that each weight loss surgery has different measures of success, percentages of weight loss by surgery, and outcomes. Dr K told me that I may have been a success with the RNY Gastric Bypass, based on the numbers, however it became clear that I did have complications associated with the gastric bypass. I was scheduled for an Endoscopy the next week, which Dr. K performed. The endoscopy confirmed that I had a Gastro-gastric Fistula. Simply put, this was an abnormal connection between the bypassed stomach and the small pouch created by the RNY Gastric Bypass surgery. Food could travel two ways, thus rendering the Gastric Bypass ineffective, and causing weight gain.
Dr. Keshishian performed a revision to the Duodenal Switch Surgery on May 31, 2013. This procedure corrected my anatomy, enabling me to lose weight and regain my health once again. I have had wonderful success and I have lost 104 pounds. More importantly, I do not have the complication of the dumping syndrome, episodes of nausea and vomiting and am leading a normal life. I am not prisoner to my weight, what I can and cannot eat or the fear of weight gain.
")
I contacted Dr. Ara Keshishian, in Glendale, and had a consultation that week. Meeting “Dr. K” was amazing! It was the first time a Doctor did not blame me for my weight. He explained that each weight loss surgery has different measures of success, percentages of weight loss by surgery, and outcomes. Dr K told me that I may have been a success with the RNY Gastric Bypass, based on the numbers, however it became clear that I did have complications associated with the gastric bypass. I was scheduled for an Endoscopy the next week, which Dr. K performed. The endoscopy confirmed that I had a Gastro-gastric Fistula. Simply put, this was an abnormal connection between the bypassed stomach and the small pouch created by the RNY Gastric Bypass surgery. Food could travel two ways, thus rendering the Gastric Bypass ineffective, and causing weight gain.
Dr. Keshishian performed a revision to the Duodenal Switch Surgery on May 31, 2013. This procedure corrected my anatomy, enabling me to lose weight and regain my health once again. I have had wonderful success and I have lost 104 pounds. More importantly, I do not have the complication of the dumping syndrome, episodes of nausea and vomiting and am leading a normal life. I am not prisoner to my weight, what I can and cannot eat or the fear of weight gain.
Medical Advice and Social MediaExclusive Member Content
June 10, 2014 5:31 pm
Protein Metabolism Optimization
June 09, 2014 5:08 pm
It’s confusing out there in the world of protein supplements and nutrition. Hopefully we can clear up some of the information with this blog post. Part I will be about protein utilization and supplementation and Part II will be about Protein Energy Malnutrition (PEM). So let’s get started with the basics of protein utilization and metabolism. This will clarify what our goals are and what we need to achieve them.

Protein Metabolism:
There are 23 Amino Acids (AA) that combine to form peptide chains. These peptide chains link together to make polypeptides, which are the building blocks of many proteins sources. These types of proteins are called proteinogenic.
Essential vs Non-essential:
Nine of these proteinogenic AA’s are essential meaning that the human body cannot make them. They must be taken in by food sources. The other AA’s are considered non-essential because the body can produce these without an outside food sources.
Complete Protein vs Incomplete Protein:
A complete protein contains all of the essential amino acids and an incomplete protein does not have all nine of the essential amino acids.
|
Essential Amino Acids
|
Non-essential Amino Acids
|
|
Leucine
|
Alanine
|
|
Isoleucine
|
Arginine
|
|
Valine
|
Asparagine
|
|
Histidine
|
Aspartic Acid
|
|
Lysine
|
Cysteine
|
|
Methionine
|
Glutamic acid
|
|
Phenylalanine
|
Glycine
|
|
Threonine
|
Ornithine
|
|
Tryptophan
|
Proline
|
|
Selenocysteine
|
|
|
Serine
|
|
|
Tyrosine
|
|
|
Threonine
|
|
|
Glutamine
|

Branched Chain Amino Acids (BCAA’s) are an incredibly important subgroup of the essential Amino Acids. Three of the nine essential AA’s are BCAA’s. They are leucine, isoleucine and valine. These three AA’s make up 40% of the protein required by humans. Muscle protein is made up of 35% of these three BCAA’s. Any protein supplement after weight loss surgery should contain these three amino acids, Isoleucine, Leucine and Valine.
Protein breakdown begins in the stomach with the addition of enzymes and acid then continues into the small bowel where absorption takes place. Protein must be broken down by these enzymes and acid to single Amino Acids or peptide chains no longer the 4 AA’s in order for the intestinal absorptive cells to absorb the protein. The 4 chain peptide chains are further broken down within the intestinal absorptive cells.
Protein absorption takes place easily but the most important factor is protein utilization. Protein utilization is how much of the protein ingested is actually utilized by the body. The body may absorb a great deal of a protein food source but can only utilize about 30-40g of a high quality protein source at a time. The body does not store protein as it does with other nutrients. Therefore, whatever the body doesn’t utilize is metabolize through the liver and converted to urea. Urea is excreted through the kidneys via urine.
Different proteins absorb at different rates, amounts and in different parts of the small bowel. i.e. Milk protein is 50% absorbed in the proximal small bowel, with 90% of the absorption taking place by the time it reaches the ileum. 1 It’s important to understand this because of the rearranging of the small bowel in the Duodenal Switch. Protein is no longer being exposed to the mucosa of the proximal small bowel due to the altered anatomy of the duodenal switch. This altered anatomy results in much lower absorption of protein, thus the increase levels of protein one needs to consume after WLS. Post WLS the body will compensate and increase protein absorption in the other areas of the small bowel. This may also explain why some weight is regained several years after WLS. 2
Reduced protein absorption is why Bioavailability or Biological Value (BV) is so important when deciding on a protein source. Biological Value is the measure of how efficiently the body utilizes the protein from the food source. You will find this BV number on some protein supplemental products. The higher the BV numbers the better utilization of the protein source by the body. Whey protein and egg protein are considered the highest BV. The daily requirements of protein are 0.80 gram of protein per kilogram of ideal body weight calculating to approximately 50-65 grams a day. 3 However, after weight loss surgery (WLS) a person should get 80-100 grams per day, 1 gram per kilogram of weight and in some cases even higher amounts of protein.
|
Protein Type
|
Protein Biological Value
|
Net Utilization
|
Efficiency Ratio
|
|
Beef
|
80
|
73
|
2.9
|
|
Whey Protein
|
104
|
92
|
3.2
|
|
Soy Protein
|
74
|
61
|
2.2
|
|
Egg
|
100
|
94
|
3.9
|
|
Black Beans
|
0
|
0
|
|
|
Milk
|
91
|
82
|
2.5
|
|
Casein
|
77
|
76
|
2.5
|
|
Poultry
|
80
|
||
|
Fish
|
70-80
|
||
|
Brown Rice Concentrate
|
70-80
|
76
|
Adapted from: U.S Dairy Export Council, Reference Manual for U.S. Whey Products 2nd Edition, 1999 and Sarwar, 1997
Protein Supplements: First clarify the terminology in supplements.
Isolate: Is chemically purified to 90% pure protein. 100g scoop=90g protein intake. Isolates have a High BV rate.
Concentrate: 35-80% protein 100g scoop=35-80g protein intake Also contains fat, carbohydrates and in the case of Whey Concentrate, lactose. Concentrates have a high BV rate.
Blends: Combination of protein sources and purity levels. Varies in how many grams of protein are available in each product. They are lower in cost and quality in some cases. Blends have a medium/high BV rate.
Hydrolysate: enzymatically predigested for maximal speed of absorption and utilization. Very water-soluble but can have a bitter taste. Hydrolysates are high in cost and BV rate.
Branched Chain Amino Acids: contains the 3 essential AA Leucine, Isoleucine, and Valine that make up 1/3 of skeletal muscle and are vital in protein synthesis. Easily absorbed and utilized by the body. BCAA’s have a high BV rate and cost.
Animal Protein Supplements:
Animal proteins contain the 9 essential amino acids the body needs for skeletal muscle formation. It’s important to note that high fat in protein will decrease the amount of absorption and, therefore, utilization of protein due to altered anatomy after DS.
Whey Protein is a byproduct of cheese production. It has a high BV rate and is the most popular protein supplement. It is rich in muscle essential amino acids and has a fast digestion rate. It needs to be taken more often because the ease of digestion. It contains 5% lactose within the product. Whey products come in a wide variety of flavors and styles. Unflavored protein products can be added to other protein foods, such as yogurt, cottage cheese, etc. to increase the protein. Be wary of artificial sweeteners in protein supplements as they can give you unwanted side effects, such as gas or loose stool.
Whey Protein Isolate: (WPI) has one of the highest BV rates 104. WPI can be slightly more expensive but seems to be the most tolerated by WLS (weight loss surgery) patients. There are many flavors and styles with less fat and lactose than other whey protein products.
Whey Protein Concentrate: has a high BV rate 85-90. Concentrate has more fat and lactose, which may not be well tolerated by WLS patients.
Whey Protein Blends: Blends contain a mixture of both isolate and concentrate whey proteins. Which means the BV rate is higher than concentrate on it’s own. Because of increased fat and lactose this too may not be tolerated as well by WLS patients.
Casein Protein is a milk protein and has a BV rate of 91. Casein is the trigger in most milk allergies. It is more slowly digested and more filling than whey protein. It may be more difficult to tolerate after WLS.
Egg Albumin is very high in essential and nonessential AA’s. Eggs are also a great natural food source for protein. Does not have lactose but some people do have egg allergies. It is a cost effective source of protein. Supplement powders come in several flavors. This is probably nature’s perfect protein source with the highest utilization.
Goat Milk: One of the highest BCAA available food sources. Is better tolerated by people with lactose intolerance.
Beef, poultry, fish all have varied degrees of bioavailability. Please see the table above regarding each items BV rate. While beef may have a higher BV rate there may be other issues to deal with higher fat content that goes along with eating most cuts of beef. After DS higher fat content can mean looser stool or even diarrhea.
Vegetable Protein Supplements and Natural Food Sources:
Plant Protein may contain most or all essential amino acids but the amount is far less thank other protein sources particularly in the amounts of BCAA needed for skeletal muscle formation. It is best to combine or vary plant proteins to ensure adequate protein nutrition.
Soy Protein: has a BV rate of 74. It is fast digesting, lactose free and comes in a variety of flavors and unflavored. It is also cost effective and contains all the essential AA’s. Soy beans are commonly a GMO crop, so if that is concerning look for organic sources. Soy is also a high allergen food and can inhibit calcium absorbtion.
Pea Protein: 100% gluten free and lactose free. Pea protein is very easy to digest, rich in Amino Acids and is a high satiety protein. Pea Protein can be found with high levels of carbohydrate and low levels of carbohydrates. After WLS always choose lower levels of carbohydrates.
Brown Rice Isolate: BV of 70-80. Is easily digested and is a good vegan choice. Again with Brown Rice Isolate watch your carbohydrate content. Brown Rice Isolate can be chalky in texture.
Pea/Brown Rice Isolate: BV of 70-90 Combining these two gives a good profile of BCAA that rivals whey and egg proteins. It is easily digestible without allergy issues. When used in combination, rice protein and yellow pea protein offer a Protein Efficiency Ratio and BCAA’s that is comparable to dairy and egg. In addition, the texture of pea protein helps the chalkiness of rice protein.
Spirulina: Blue-green algae is easily digested and high in AA 80-95% of proteins can be digested. BUT is very allergic prone. It is also expensive and the taste can be hard to handle.
Hemp Protein: 30-50 BV rate. Hemp contains 21 amino acids and is considered a complete protein. The proteins in Hemp seeds are easily digestible, absorbed and utilized by the body. Hemp seeds are great to add to natural food products to increase protein and essential fatty acids. It is vegan friendly and low allergy rating.
Summary
So what does this all mean? It is important when looking for a protein supplement or natural food source to look for the highest bioavailable rating and BCAA levels. Most protein supplements have these listed on their labels. Read the labels on supplements to find low fat, carbohydrate and lactose for best tolerance after WLS. Consuming high amounts of fat after duodenal switch decreases the absorptive time the food products due to the altered anatomy after DS. When taking your protein it is best for absorption to have low fat to optimize your protein absorption. Be wary of artificial sweeteners in protein product. They may also cause WLS patient issues, such as increased loose stools or gas. Also, try getting trial sizes of several different supplements to see how your body tolerates the supplement and your taste. If you are not tolerating one brand of supplements try another. Isolate, Egg or Blends are best tolerated after WLS and give the highest bioavailability.
The best routine of taking your supplements after WLS is on an empty stomach in the morning or when you first wake. This is a good time to use an isolate, or blend supplement shake or natural food source such as egg. Have a midmorning protein snack or shake, lunch with high protein foods, a mid afternoon protein snack or shake, dinner of high quality protein and after dinner or as close to bedtime as you can tolerate protein supplement shake. For your meals choose the best BV rating food and also listen to what your body tolerate. Your natural food sources should be low fat, low carbohydrate and low lactose food choices. Also consider adding one of the plant protein supplements or unflavored animal supplements to your natural food sources to give an additional protein boost. The unflavored varieties can be added to nearly any food or recipe. Take care in adding protein powders to higher temperature foods, as high temperatures destroy the proteins. The key is frequent small meals and snacks with the highest quality protein. Varying your protein sources increases your chances of absorbing a variety of amino acids and nutrients.
After surgery, you should expect to be able to consume the same amount of grams of protein as the number of days post op that you are. i.e.; 30 grams of protein at the end of the first month, 60 grams of protein by 60 days post op, etc. Treat your body as you would an infant just starting to eat new foods. Try small amounts of food and only progress with a new item after several days of tolerating an old food. As always follow your surgeon’s guidelines and recommended diet. Do not progress until your surgeon has given you the go ahead.
Shared Success Story: Kerry F. had a Gastric Bypass revision to Duodenal Switch
May 27, 2014 2:12 pm
Revising from RNY to Duodenal Switch
Spending my entire life overweight, I thought I found the answer when I had my RNY gastric bypass surgery in July 2001 at the age of 24. I was 354 lbs. at 5’9 and after RNY gastric bypass lost down to my lowest weight of 192 lbs. I kept that weight off for 6 years.

Then due to my previous surgeons lack of information about vitamins (I needed an iron transfusion in 2004 due to iron deficiency anemia and malnutrition) and my ignorance of proper eating I ended up gaining 150 lbs. back in just 3 years from my intestines reabsorbing and a stretched pouch. I felt like a complete failure, embarrassed and angry. I turned to a website about putting Lap Band over bypass, a new procedure. While investigating, Dr. Keshishian I found out about revising to Duodenal Switch (DS) and how it can help lose the weight and keep it off through adherence of diet and vitamins.
I feel amazing at the age of 37 and thank Dr. Keshishian for giving my life back to me
AGAIN, always telling me from day one that I was NOT a failure – the RNY was. He also said to believe in myself, follow the plan and be proud of my accomplishments. And I am!!! My advice to all – do your research, know ALL of your options, make the best decision for you and if you want a DS revision go with one of the BEST, Dr. Keshishian. He won’t steer you wrong! I’m living proof!!!

Sunshine, Water, Rest, Air, Exercise and Diet
May 23, 2014 4:10 pm

{kind=link}
Sunshine, Water, Rest, Air, Exercise and Diet
Of course this is over simplified, but we can’t forget the importance of the basics in our general well being. Weight loss surgery and especially Duodenal Switch have distinctive supplement requirements that need to be individualized based on your individual needs.
Sunshine is essential to life. It provides the light that wakes us and helps to regulate wake/sleep cycles and provides us with a feeling of well being. Sunlight is not only the basis of all living things but crucial in boosting the bodies Vitamin D supply. Most Vitamin D deficiencies in the general public are caused by lack of sun exposure. It is important to note that our bodies can not accomplish Vitamin D metabolism if we are wearing sunscreen. Without adequate Vitamin D stores bones will not form properly, muscle strength is impaired and osteoporosis. Vitamin D 1,25(OH) accumulates in cell nuclei of the intestine, where it enhances calcium and phosphorus absorption, controlling the flow of calcium into and out of bones to regulate bone-calcium metabolism. However, after weight loss surgery this mechanism can be impaired. Addition supplementation of Vitamin D is usually required based on laboratory studies following weight loss surgery. Duodenal Switch patients should take a dry “water miscible” type of Vitamin D3 daily.
Water comprises 50-60% of our adult bodies. Water is essential in cell life. It aids in transporting vitamins, nutrients and minerals to our cells. Chemical and Metabolic reactions rely on water to remove waste products including toxins that the organs’ cells reject and removes them through urine and feces. Our body temperature is regulated by sweating and the evaporation of water on the skin. Also, effectively Lubricating our joints and acting as a shock absorber for our brain, eyes, and spinal cord. Decreased stomach size, after weight loss surgery, limits the amount of water a person can drink at one time. It is imperative that patients ingest enough waters and fluids after surgery. We like to see our patients consume a minimum of 64 ounces of fluids a day, more on warmer days.
Rest is something we can all use more of. Lack of sleep can cause a whole host of health issues ranging from altered levels of hormones involved in metabolism, appetite regulation, stress response to cardiovascular health, insulin resistance, immune function and most importantly post-operatively tissue repair, muscle growth and protein synthesis. It’s easy to take rest for granted but do not underestimate the power of sleep.
Air is an obvious essential of life. It is important in about every function of our cells. After surgery it is important to lung health and tissue repair. Be aware of the type of air you are breathing. Pollution and contaminants in the air can impair lung function. After surgery your breathing and breathing exercises will prevent complications such as pneumonia and atelectasis. Long term air contaminants can cause asthma and long term lung health. In addition, post surgical patients will need to use their incentive spirometers to combat lung complications.
Exercise’s health benefits can not be denied. Exercise combat health conditions and disease such as stroke, metabolic syndrome, diabetes and cardiovascular disease. It also improves emotional outlook and mood. Physical activity stimulates the brain to release chemicals that involve increasing memory function. Exercise helps maintain healthy weight, improves energy, promotes better sleep, lowers stress and anxiety. Needless, to say after surgery exercise is extremely important for all the above reasons but also to ward off complications such as pulmonary embolism and deep vein thrombosis.
Diet is last but definitely not least. Balance along with moderation and eating whole unprocessed foods are best ways to ensure your health. We derive most our building blocks for cell growth from the nutrients we consume. The quality of the food we put into our bodies is important in lowering health risks such as cardiovascular disease, cancer, and weight control. Protein is crucial in muscle growth, hemoglobin, cell structure and enzymes formation. It is extremely important after weight loss surgery to remain diligent about protein intake throughout your lifetime.
It is interesting to see how all these elements are so intertwined in their synergy to maintain health. Most are easily found or done in nature. When engaging in one of these elements, many of the others are needed or benefited by the doing the first. Exercise requires that you stay hydrated, deep breath, possibly out in the sunlight and therefore you will rest better. Always follow your surgeon’s orders and recommendations based on your individual health status and laboratory studies.