
Cheers! Alcohol Metabolism
December 17, 2024 1:59 pm
Cheers! Let’s take a minute to look at alcohol metabolism. It’s that time of year when it seems we are going from one Holiday or Christmas party to another, and then we get together with the family and have a little more alcohol. The following diagram shows how alcohol metabolism takes place.
Alcohol is a caloric intake, and we all need to keep close tabs on it. Alcohol is very easily metabolized and the calories add up quickly. Every stage of alcohol processing in the liver involves the extraction of calories and free radicals, which are toxins. Excess calories not used in bodily functions can be stored as fat mass. Alcohol can be a roadblock in weight loss. Those drinks add up!


Here is a short video as a reminder while everyone waits to get ready for the next party.
Happy holidays.
A newsletter post from 2004 regarding the effects of alcohol and weight loss surgery.
Vitamin Toxicity
December 17, 2024 1:36 pm
Patients are frequently asked to explain why they take high fat- or water-soluble vitamin doses. They are have often been scared by their well meaning healthcare providers that their higher levels of vitamin supplements will end up with vitamin toxicity.
Let’s clarify one point: there is such a thing as too much vitamin.
However, the point that is often overlooked, throughout teaching within professional schools (medical, nursing, pharmacy, etc.) and drug manufacturers, is recommendations are based on “how much to take” and not how much is needed to keep a patient’s blood level in the normal range.

This table highlights how toxicity is described and what requirements are recommended. Vitamin toxicity is seen rarely in post-weight loss surgical patients who take them proactively in as many doses as needed to get their blood levels in the normal range. I see more patients in the office who suffer from low vitamin levels, such as vitamin D and A levels (duodenal switch and sleeve), than any patient with high or toxic levels of any vitamins.
Here is an example of critical vitamin A deficiency and night blindness and how, with aggressive large-dose supplementation, her condition was corrected.
Too Much Protein & Protein Metabolism
December 17, 2024 12:40 pm
 The key is to manage the delicate balance of taking adequate protein against what is needed to maintain healthy muscle mass and immune function. The image below shows what happens when patients do not consume sufficient protein over long periods. The body starts breaking down the muscles and converts this all to energy. In this diagram, body proteins are the muscle mass broken down into amino acids to supply the body with needed glucose and ketones to give the body energy for its functions.
The key is to manage the delicate balance of taking adequate protein against what is needed to maintain healthy muscle mass and immune function. The image below shows what happens when patients do not consume sufficient protein over long periods. The body starts breaking down the muscles and converts this all to energy. In this diagram, body proteins are the muscle mass broken down into amino acids to supply the body with needed glucose and ketones to give the body energy for its functions.
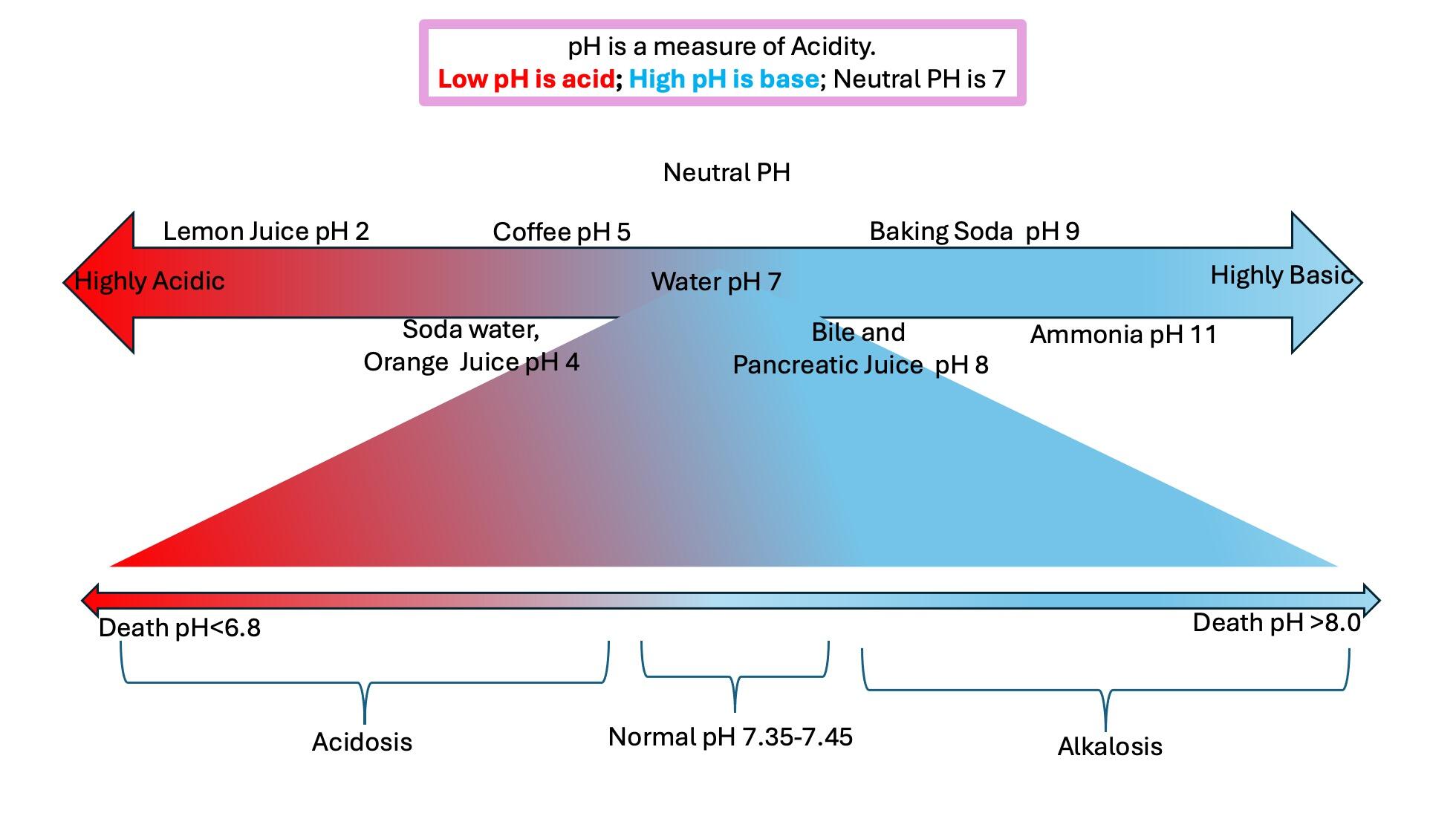
Digestive Juices
December 16, 2024 9:04 am
A patient story: Lap Band complication and Wegovy
October 24, 2024 4:30 pm
Not too long ago, I saw an old patient who had seen me years ago after having had a lap band placed for weight loss. At the time, I recommended that the lap band be removed and that alternative plans be made. I suspected a slipped band. We discussed the reality that after the band removal, weight gain is to be expected. Several surgical options were discussed, and the patient dismissed them as “too radical.” The patient decided to “deal” with the ongoing nausea and vomiting since it was a small price to pay for the weight loss. I warned the patient that elective removal of the band is much safer than an emergency procedure in the middle of the night when it is least convenient. The patient did end up with an emergency lap band removal and was started on GLP-1 Agonists (Wegovy) because of the weight gain that followed the band removal. The side effects of the medication were debilitating, with nausea, dizziness, and fainting due to low blood sugar. The drug has all been stopped, and most, not all, of the side effects are resolved. The plan is to get this patient in a better shape and, reevaluate the esophagus and the stomach, and formulate a strategy based on the blood work, upper endoscopy, upper GI study findings and decide if the patient will be a good candidate for the Laparoscopic sleeve or the duodenal switch operation.
Here are my recommendations:
- Patients should avoid lap bands. Those with lap bands, regardless of how they feel and whether they are having issues with them, should have the lap band removed immediately before they end up in the emergency room or have irreversible changes to the cells or function of the stomach and esophagus.
- Patients who have the lap band removed will have less weight loss with the sleeve than those who have the sleeve as the primary procedure (the lesson here is that a less invasive, seemingly easy solution is much worse long term; more on this below). Lap Band patients should be revised to the duodenal switch, SPIS, SADI, or Gastric bypass if they have substantial weight to lose.
- GLP-1 agonist medication should be avoided. It is not a solution to the underlying problem but a band-aid covering the metabolic derangement.
- GLP-1 agonist medication needs to be taken long term, and there is no exit strategy– when the patients stop taking the drug, the weight comes back, in addition to the complication associated with it.
- I have also heard that “if it were bad, then the FDA would not approve it.” well, let’s think about it: the FDA approved the Lap band and Phen-Fen, and we all know how these worked out.
- There are no shortcuts, simple injections, or a pill for the complex, multifaceted condition of obesity. Advocating solutions with no long-term outcome, significant complications, and safety concerns is irresponsible.
- A diabetic patient should take the medication LIFELONG to control their blood sugars, including the GLP-1 agonist class of drugs. The concerns are for these medications being used for the treatment of obesity

Radiology film of normal position and a slipped LapBand
SUMMARY: Buyers beware- those who choose to embark on the dangerous load of GLP-1 agonist medications should be prepared to deal with the short and long-term complications of the medication and its withdrawal. This is like the problems that are being seen with patients who choose to have a lap band because it was advocated as simple, reversible, and the Phen fen medication for weight loss with the associated cardiac complication.
https://www.dssurgery.com/wp-content/uploads/2024/09/P000008S017b.pdf
https://www.dssurgery.com/wp-content/uploads/2024/09/20-year-all-procdure-metaanalysis.pdf
https://www.dssurgery.com/weight-loss-injection/
https://www.dssurgery.com/glp-1/
https://www.dssurgery.com/weight-loss-medications-compared-to-surgery/
https://www.dssurgery.com/articles/glp-1-agonists-a…agency-clinicians/
https://www.dssurgery.com/articles/managing-the-gas…clinical-practice/Should Adjustable Gastric Banding (Lap Band) be done?
October 06, 2024 9:17 pm
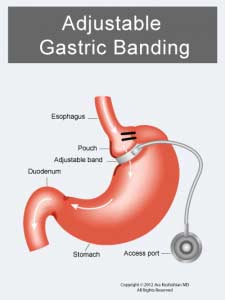 The Lap Band was approved in the US in 2001 (BMI> 40). The following studies used only small samples and examined short-term efficacy and safety. They were then performed to consider the utility of the Laob band for patients with lower BMI (BMI 30-40).
The Lap Band was approved in the US in 2001 (BMI> 40). The following studies used only small samples and examined short-term efficacy and safety. They were then performed to consider the utility of the Laob band for patients with lower BMI (BMI 30-40).  Noe the frequent complications of nausea, difficulty swallowing, pain, and reflux-which may sound familiar to a lot of patients who have had and still have the Lap Band.
Numerous US and international studies have been published over the years, including short-term and long-term studies. The summary outcome has been the same, with only a few exceptions.
Noe the frequent complications of nausea, difficulty swallowing, pain, and reflux-which may sound familiar to a lot of patients who have had and still have the Lap Band.
Numerous US and international studies have been published over the years, including short-term and long-term studies. The summary outcome has been the same, with only a few exceptions.
- The Lap Band does not result in long-term sustained weight loss.
- Lap band has significant complications, some of which may not be reversible.
- The lap band can be removed, but eroding the banc to the stomach is not easy.

Surgery Bests Lifestyle Changes, GLP-1 for Durable Weight loss
September 11, 2024 9:04 pm

SAN DIEGO-Bariatric surgery far outperforms lifestyle interventions and glucagon-like peptide-1 (GLP-1) medications at maintaining weight loss, according to a meta-analysis presented at the 2024 annual meeting of the American Society for Metabolic and Bariatric Surgery.
With results from six randomized controlled trials, three systematic reviews, and more than 40,000 patients, the study is the first synthesis of its kind.
“The analysis included two systematic reviews of bariatric surgery, one of Roux-en-Y gastric bypass including8,665 patients and one of sleeve gastrectomy including 6,095 patients: a single systematic review or lifestyle interventions including 723 patients; and six randomized controlled trials of GLP-1 medications, including four studies of semaglutide with a total of 11,871 patients and two of tirzepatide with 3,209 patients.
Lifestyle interventions were the least effective treatment, the investigators found, producing a mean total body weight loss of 7.4% at the end of the treatment period, followed by a mean per-month weight regain of 0.14%, with participants reaching their pre-intervention weights within 4.1 years.
GLP-1 medications proved more effective. Weekly semaglutide injections for 20 weeks and tirzepatide for 36 weeks produced a mean total body weight loss of 10.6% and 21.1%, respectively. Roughly half of the weight lost was regained within a year after stopping injections; with continued injections, weight loss plateaued after 17 to 18 months, at 14.9% for semaglutide and 22.5% for tirzepatide.
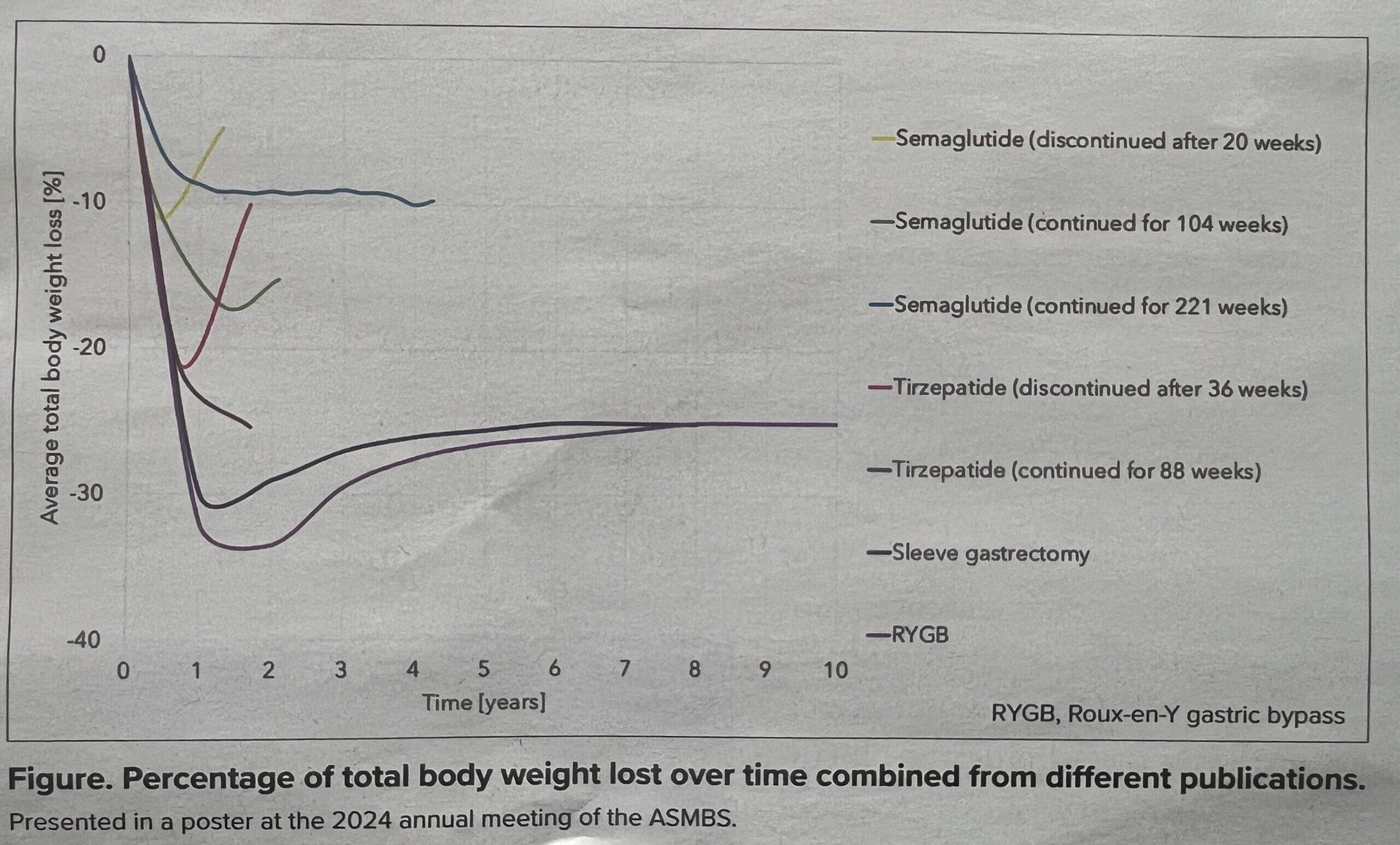
Outcomes after surgery were significantly better. Gastric bypass surgery and sleeve gastrectomy resulted in a mean total body weight loss of 31.9% and 29.5%, respectively, one year after surgery. Accounting for weight regained in the decade after surgery, both procedures produced a stable total body weight loss of approximately 25%.
While the results demonstrate a striking difference favoring surgery, lead investigator Megan Jenkins, MD, a bariatric surgeon at NYU Langone Medical Center in New York City, emphasized that surgery and medication ought to be viewed not in opposition but through a holistic lens as options and potential complements based on the needs of each patient.
“One of the big benefits of these new medications is that it’s helped us to treat obesity as a chronic disease,” Dr. Jenkins said. “We’ve always treated it that way, but I think the medical field has had trouble truly seeing it as a chronic disease. Like diabetes and high blood pressure, for example, which have always been treated with a combination approach.
Bile Reflux Gastritis
August 02, 2024 10:53 am
Bile Reflux
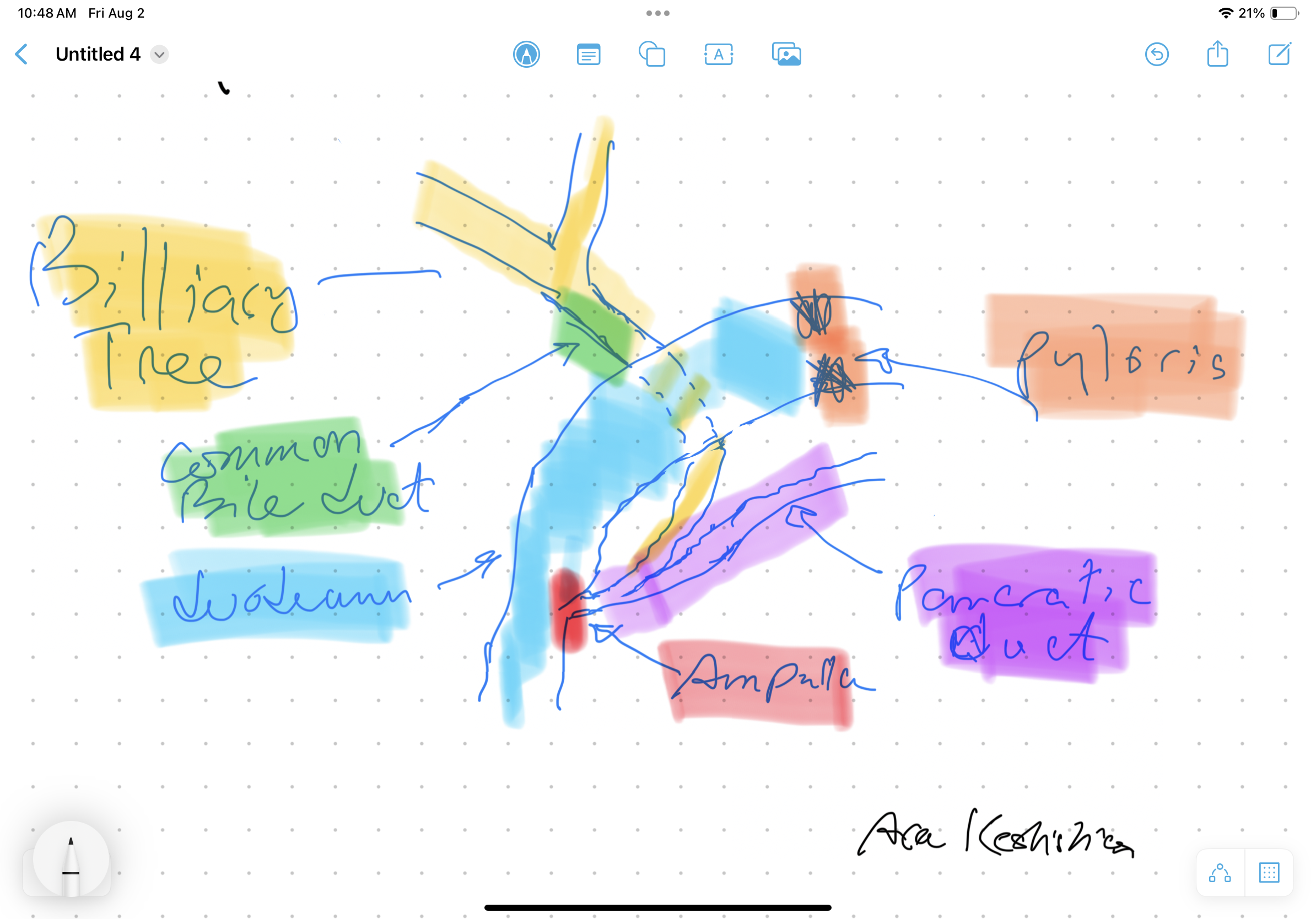
Bile Reflux is primarily a diagnosis of exclusion. All other possible causes must be ruled out, and bile reflux gastritis is made with the pertinent symptoms. The reason for this is that there is no primary test that can prove the diagnosis. When it comes to treatment, the surgical option requires preventing the bile from coming back to the stomach. The procedure we have performed routinely for bile reflux gastritis is the duodenal switch (without a reduction in the stomach size). This allows the food to go through an intact stomach and pyloric valve with normal stomach physiology (to prevent dumping syndrome). The bile is diverted through 100 cm of the small bowel as the biliary and alimentary limbs to prevent backflow of bile to the stomach (if it’s made too short). The procedure referenced (https://www.americanjournalofsurgery.com/article/S0002-9610(03)00213-7/abstract) is nearly 20 years old. It is rarely, if at all, performed due to its very complex and relatively high-risk nature. Its primary role for a surgeon is to reconstruct the biliary track flow. This operation involved transecting the common bile duct and creating a biliary tree to small bowel anastomosis. This is, at times, done when there is injury, obstruction, or tumor of the bile duct. This anastomosis has its complications, including stricture and sump syndrome. Therefore, hepaticojejunostomy or hepato-duodenostomy anastomosis are reserved for cases with no alternatives. A-Normal Anatomy
B-Duodenal switch for bile Reflux
C-Hepatojejunostomy for bile relaxation was proposed in a 2003 study.
A-Normal Anatomy
B-Duodenal switch for bile Reflux
C-Hepatojejunostomy for bile relaxation was proposed in a 2003 study.

Weight loss Medications compared to surgery
February 20, 2024 5:44 pm

SIPS-SADI and ASMBS
December 31, 2023 1:21 pm