
Bile Reflux
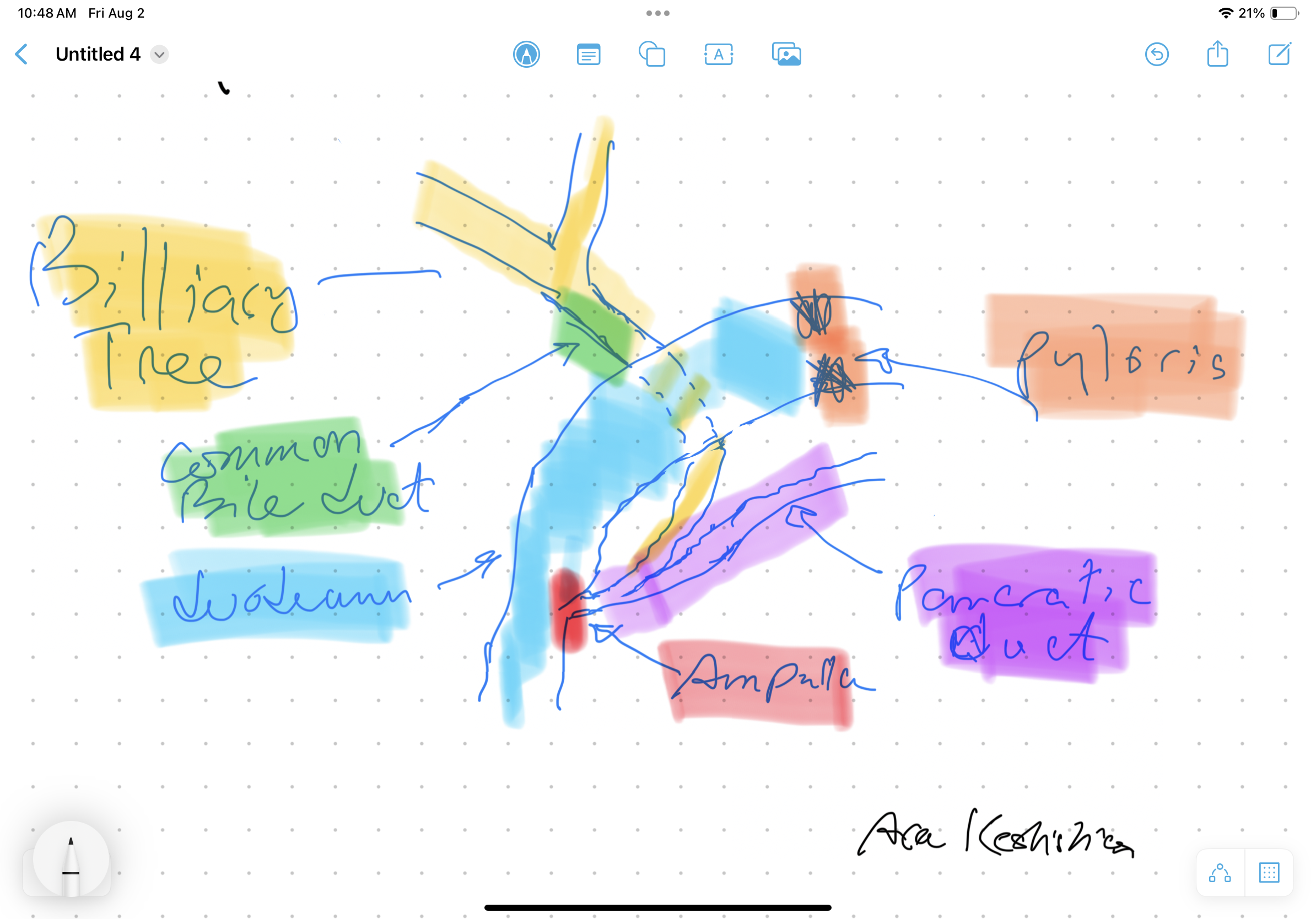
Bile Reflux is primarily a diagnosis of exclusion. All other possible causes must be ruled out, and bile reflux gastritis is made with the pertinent symptoms. The reason for this is that there is no primary test that can prove the diagnosis. When it comes to treatment, the surgical option requires preventing the bile from coming back to the stomach. The procedure we have performed routinely for bile reflux gastritis is the duodenal switch (without a reduction in the stomach size). This allows the food to go through an intact stomach and pyloric valve with normal stomach physiology (to prevent dumping syndrome). The bile is diverted through 100 cm of the small bowel as the biliary and alimentary limbs to prevent backflow of bile to the stomach (if it’s made too short). The procedure referenced (https://www.americanjournalofsurgery.com/article/S0002-9610(03)00213-7/abstract) is nearly 20 years old. It is rarely, if at all, performed due to its very complex and relatively high-risk nature. Its primary role for a surgeon is to reconstruct the biliary track flow. This operation involved transecting the common bile duct and creating a biliary tree to small bowel anastomosis. This is, at times, done when there is injury, obstruction, or tumor of the bile duct. This anastomosis has its complications, including stricture and sump syndrome. Therefore, hepaticojejunostomy or hepato-duodenostomy anastomosis are reserved for cases with no alternatives. A-Normal Anatomy
B-Duodenal switch for bile Reflux
C-Hepatojejunostomy for bile relaxation was proposed in a 2003 study.
A-Normal Anatomy
B-Duodenal switch for bile Reflux
C-Hepatojejunostomy for bile relaxation was proposed in a 2003 study.

Recent Posts
- Cheers! Alcohol Metabolism December 17, 2024
- Vitamin Toxicity December 17, 2024
- Too Much Protein & Protein Metabolism December 17, 2024
- Digestive Juices December 16, 2024
- A patient story: Lap Band complication and Wegovy October 24, 2024
Leave a Reply